Female Anatomy Flashcards
what are the 6 different functions of the bony pelvis?
support of upper body when sitting and standing
transference of weight from vertebral column to the femurs to allow standing and walking
attachment of muscles of locomotion and abdominal wall
attachment for external genitalia
protection of pelvic organs, their blood and nerve supplies, their venous and lymphatic drainage
passage for childbirth
the bony pelvis consists of what 3 structures?
2 hip bones
sacrum
coccyx
*coccyx not part of pelvic girdle

each hip bone is a fusion between which three structures?
ilium
ischium
pubis
*ischium and ilium fused from age 4-5, these do not fuse with pubis until puberty

identify the following structures within the ilium:
a) iliac crest
b) iliac fossa
c) ASIS
d) PSIS

identify the following structures within the ischium:
a) ischiopubic ramus
b) ischial tuberosity
c) ischial spine

identify the following structures within the pubis:
a) ischiopubic ramus
b) pubic arch
c) sub-pubic angle
d) pubic tubercle
e) superior pubic ramus

what are the contents of the pelvis inlet?
sacral promontory
ilium
superior pubic ramus
pubic symphysis

what are the contents of the pelvic outlet?
pubic symphysis
ischiopubic ramus
ischial tuberosities
sacrotuberous ligaments
coccyx

what is the space within the bony pelvis which lies between the pelvic inlet and pelvic outlet called?
pelvic cavity

the pelvic cavity lies continuous with abdominal cavity above, but what separates the pelvic cavity from peroneum?
pelvic floor
name the palpable surface landmarks of the pelvis?
*the inguinal ligament attaches between the ASIS and pubic tubercle

identify the structures of the bony pelvis on x-ray images?

identify the location of the following joints within the pelvis:
a) sacroiliac joint
b) hip joints (synovial)
c) pubic symphysis (secondary cartilaginous)

what are the two ligaments within the pelvis that we must know?
*there are a large number
sacrotuberous ligaments
sacrospinous ligaments
*these ensure the inferior part of the sacrum is not pushed superiorly when weight is suddenly transferred vertically through vertebral column (eg when jumping or during late pregnancy)

do these ligaments constrict or relax during late pregnancy?
relax
which two foraminae do the sacrotuberous and sacrospinous ligaments form?
greater and lesser sciatic foraminae

what is the obturator canal?
area of obturator foramen which is not covered by obturator membrane
contains obturator nerve and vessels

why do pelvic fractures tend to be multiple or combined with joint dislocation?
it is very hard to break a ring in just one place
identify vessels within the bony pelvis which can cause life threatening haemorrhage and/or damage to pelvic organs during trauma?

identify the difference between the male and female pelvis?
male = left
female = right (AP and transverse diameters are larger both at pelvic inlet and outlet. The subpubic angle and arch is wider. The pelvic cavity is also more shallow)

what is “moulding”?
the movement of one bone over another to allow the foetal head to pass through pelvis. The presence of the sutures and fontanelles (soft spots) allows bones to do this

what is the “vertex” of the foetal skull?
an area of the skull outlined by anterior and posterior fontanelles and parietal eminences. Important during childbirth to identify where head is lying

what is the difference between the occipitofrontal and biparietal diameters of foetal skull?
the occipitofrontal diameter is longer then the biparietal diameter (ie head is longer than it is wide)

giving that the transverse diameter of the pelvis is wider than AP diameter (female) and also that the occipitofrontal diameter is longer than biparietal diameter (foetus), how should foetus enter pelvic cavity?
facing either to the right or left (transverse) direction
*the distance of the foetal head from the ischial spines is referred to as the “station”. A negative number means the head is superior to the spines, and a positive number means the head is inferior to the spines
during childbirth, how should the foetal head be positioned at the following structures:
a) pelvic inlet
b) descending through pelvic cavity
c) pelvic outlet
a) pelvic inlet = head should be transverse
b) descends through pelvic cavity = head should rotate and it should be flexed
c) pelvic outlet = the foetal head should lie occipitoanterior (OA) and extension of head on the neck should occur

once the babies head has been delivered, there is further rotation - true or false?
true - further rotation so that shoulders and rest of baby can be delivered

what structures are contained within the pelvic cavity?
ovaries
uterine tubes
uterus
superior part of vagina

what structures are contained within the perineum?
inferior part of vagina
perineal muscles
bartholin’s glands
clitoris
labia

what does the inferior part of the parietal peritoneum form?
floor of peritoneal cavity and a roof over pelvic organs
what is the role of the peritoneum?
covers superior aspect organs
forms pouches = vesico-uterine (utero-vesico) and recto-uterine (pouch of douglas)

why does excess (abnormal) fluid within the peritoneal cavity tend to collect within the pouch of douglas and how can this be drained?
because it is the most inferior part of the peritoneal cavity in the anatomical position (in female)
fluid collection can be drained via a needle passed through the posterior formix of the vagina
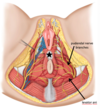
identify different areas of the peritoneum from a superior view of the female pelvis?

what is the broad ligament of the uterus and what is its function?
double layer of peritoneum which extends between the uterus and the lateral walls and floor of the pelvis
helps maintain the uterus in its correct midlin eposition (contains uterine tubes and proximal part of round ligament)

the uterus is held in position by which 3 levels of support?
what can weakness of these supports result in?
number of strong ligaments (eg uterosacral ligaments), endopelvic fascia and muscles of the pelvic floor (eg levator ani)
weakness can result in uterine prolapse (movements of uterus inferiorly)

what is the most common position of the uterus?
anteverted (cervix tipped anteriorly relative to the axis of the vagina) and anteflexed (uterus tipped anterior relative to the axis of the cervix - the mass of the uterus lies over bladder)

what is the normal variation in the position of the uterus?
retroverted (cervix tipped posterior relative to axis of vagina) and retroflexed (uterus tipped posteriorly relative to axis of cervix)

what area of the cervix is sampled during a smear test?
the squamo columnar junction (transformation zone)
where does fertilisation occur?
the ampulla

what is a bilateral salpingo-oophrectomy?
removal of both uterine tubes and ovaries
what is the communication between the genital tract and the peritoneal cavity?
what is the clinical implication of this?
the fimbriated end of the uterine tubes open into the peritoneal cavity
in theory, infection could pass between the two (PID can cause peritonitis and ectopic pregnancy can develop in peritoneal cavity)
on a hysterosalpingogram (HSG), what does radiopaque dye spilling out of the end of the uterine tube and into the peritoneal cavity suggest?
that the tube is patent

where do the ovaries develop?
on the posterior abdominal wall
they then move onto the lateral wall of the pelvis
in post-pubertal females, where is an ovum released into?
the peritoneal cavity to be picked up by the fimbriae of uterine tube
where is the only space in the vagina where the walls are not in contact?
superior where the cervic holds them apart forming a fornix
the fornix has 4 parts - anterior, posterior and two lateral

what must be palpated during a vaginal digital examination?
ischial spines (laterally at 4 and 8 oclock)
uterus (by bimanual palpation)
adnexae (uterine tubes and ovaries by placing fingers into latral fornix and pressing deeply with other hand in iliac fossa of same side - can detect large masses or tenderness)

pelvic diaphragm forms the floor / roof of what?
floor of pelvis
roof of perineum
what do the openings in the pelvic floor allow for?
passage of the distal parts of alimentary, renal and reproductive tracts from pelvis to perineum

what type of muscle is the levator ani?
what is its role and nerve supply?
skeletal muscle - voluntary control
forms majority of pelvic diaphragm and provides continual support for the pelvic organs
supplied by “nerve to levator ani” - S3, 4 and 5 sacral plexus

what supplies the perineal muscles?
pudendal nerve
what is the perineal body?
why is it important and when can it be distrupted?
bundle of collagenous and elastic tissue into which perineal muscles attach
it is important to pelvic floor strength, can be disrupted during labour and is located just deep to skin
identify the location of the bartholins gland (secrete mucus to lubricate vagina)?

identify the surface anatomy of the female perineum?

what is the anatomical location of the female breast?
bed of breast extends from rib 2-6 and lateral border of sternum to mid-axillary line
lie on deep fascia covering pec major and serratus anterior
retromammary space lies between fascia and breat
firmly attack to skin via suspensory ligaments

how should a lump in the female breast be assessed?
assess whether it is fixed to any underlying tissue eg pectoral fascia by asking patient to place her hands firmly on her hips (in doing so there is contraction of pectoral muscles)
both the axilla and supraclavicular area should be assessed

where does most lymph from the breast drain to?
the ipsilateral axillary lymph nodes and then to supraclavicular nodes (75%)
*lymph from inner breast quadrants can drain to parasternal lymph nodes
*lymph from lower inner breast quadrant can drain into abdominal lymph nodes

breast surgeons use “levels” of axillary nodes to descrive the extent of axillary node clearance and the position of each level can be described in relation to pectoralis major - what are these levels?
level I - inferior and lateral to pectoralis major
level II - deep to pectoralis major
level III - superior and medial to pectoralis major

identify the blood supply and drainage of the breast?

what structure seperates the pelvis and the perineum?
levator ani muscle
- above = pelvis
- below = perineum

what is the flow of the different types of autonomic nerves of the pelvis?
sympathetics = sacral sympathetic trunks -> T11-L2 -> superior hypogastric plexus
parasymathetics = sacral outflow (S2,3,4) -> pelvic splanchnic nerves -> emerge from spinal roots and mixes with sympathetics in inferior hypogastric plexus

describe a summary flow chart of the pain sensation within the female?

what are the three different types of anaesthesia?
spinal anaesthetic (anaesthetises from waist down - intra and subperitoneal plus somatic areas)
epidural anaesthetic (anaesthesities sub-peritoneal plus somatic areas innervated by pudendal nerve)
pudendal nerve block (anaesthetises area innervated by pudendal nerve)

what spinal level is spinal and epidural anaesthetic injected?
L3-L4 (L5) region
*cauda equina begins at L2 and subarachnoid space ends at level of S2

what structures does the needle need to pass through during an epidural anaesthetic?
supraspinous ligament
interspinous ligament
ligamentum flavum
epidural space (fat and veins)

what structures does the needle need to pass through in spinal anaesthetic?
supraspinous ligament
interspinous ligament
ligamentum flavum
epidural space (fat and veins)
dura mater
arachnoid mater - then reaches CSF in subarachnoid space

how do those spinal nerves below L2 recieve sympathetic fibres?
sympathetic ganglia receive fibres from L2 level via the sympathetic chain
and distribute them via connections with lumbar, sacral and coccygeal spinal nerves

what type of nerve fibres does the pudendal nerve contain?
somatic motor and somatic sensory
it is a branch of the sacral plexus (S2, S3 and S4)

what is the course of the pudendal nerve which makes it identifiable?
exits pelvis via greater sciatic foramen, passes posterior to sacrospinous ligament, crosses the lateral aspect of the sacrospinous ligament, and re-enters pelvis / perineum via lesser sciatic foramen
it travels in pudendal canal (passageway within obturator fascia with the internal pudendal artery and vein and the nerve to obturator internus)
branches to supply structures of perineum

what can be used as a landmark to administer pudendal nerve block?
ischial spine

during labour, the branches of the pudendal nerve can be stretched with the resultant stretch of the nerve fibres
fibres within which muscles could be torn as a result?
levator ani (puborectalis) or external anal sphincter could be torn and as a result, the muscle weakened (1st degree, 2nd degree, 3rd degree)

what type of incision is used for an episiotomy?
posterolateral (mediolateral) incision
made into the relatively safe fat filled ischioanal fossa and avoids the incision extending into the rectum
*medial incision not often used as if further tearing occurs, it is going to involve tha anal sphincter

what are common surgical incisions in O&G?
lower segment caesarean section (LSCS)
laparotomy
abdominal (and vaginal) hysterectomy
laparoscopy (use langer lines)

identify the different layers of the anterolateral abdominal wall?

where does the external obliques attach and in which direction does their fibres run?
attach between lower ribs and iliac crest, pubic tubercle and linea alba (midline blending of aponeuroses)
fibres run in same direction as extenal intercostals

where do the internal obliques attach and in which direction do their fibres run?
attach between lower ribs, thoracolumbar fascia, iliac crest and linea alba
fibres run in same direction as internal intercostals

where to the transversus abdominis attach?
between lower ribs, thoracolumbar fascia, iliac crest and linea alba

what divides each rectus abdominis into 3 or 4 smaller muscles and works to improve mechanical efficiency?
tendinous intersections

what forms the linea alba?
interweaving of rectus abdominis aponeuroses which runs from the xiphoid process to the pubic symphysis

what is the rectus sheath?
combined aponeuroses of anterolateral abdominal wall muscles which lies immediately deep to superficial fascia
it surrounds the rectus abdominus muscles and is a strong, fibrous layer

identify the different layers of the internal surface of the abdominal wall?

describe the nerve supply to the anterolateral abdominal wall?
enters from lateral direction
7th - 11th intercostal nerves become the thoracoabdominal nerves
subcostal (T12), iliohypogastric (L1) and ilioinguinal (L1) also supply this area
they travel in plane between internal oblique and transversus abdominis

what arteries supply the anterior abdominal wall?
superior epigastric arteries (continuation of internal thoracic which emerges at superior aspect of abdominal wall and lies posterior to rectus abdominis)
inferior epigastric arteries (branch of external iliacs which emerges at inferior aspect of abdominal wall and lies posterior to rectus abdominis)

what is the blood supply to the lateral abdominal wall?
intercostal and subcostal arteries which are continuations of posterior intercostal arteries and emerge at lateral aspect of abdominal wall

in which way do you incise muscle in order to minimise traumatic injury?
incise in the same direction as muscle fibres - avoids damaging nerves and interrupting blood supply

during an LSCS, the rectus muscles are cut - true or false?
false - they are not cut
instead, they are separated from each other in a lateral direction, moving them towards their nerve supply

during a LSCS, what layers do you open and which ones do you stitch close again?
layers when opening = skin and fascia, anterior rectus sheath, rectus abdominis (separate the muscles), fascia and peritoneum, retract bladder (catheter usually already inserted), uterine wall and amniotic sac
layers to stitich closed = uterine wall with visceral peritoneum, rectus sheath, (fascial layer if increased BMI), then skin

what type of incision is performed during a laparotomy?
midline incision
this is relatively bloodless which means that healing is not as good and increases the chance of wound complications eg dehiscence, incisional hernia

what type of incision is used for a laparoscopy?
a sub-umbilical incision
when viewing pelvic orgams, the position of uterus can be manipulated by grasping the cervix with forceps inserted through the vagina

during a laparoscopy, if a lateral port is required then care must be taken to avoid what artery?
the inferior epigastric artery
this is a branch of the external iliac artery which emerges just medial to deep inguinal ring (located halfway between ASIS and pubic tubercle) and passes in a superomedial direction posterior to rectus abdominis

what is the difference between an abdominal hysterectomy and a vaginal hysterectomy?
abdominal - removal of uterus via an incision in the abdominal wall (suprapubic incision)
vaginal - removal of uterus via the vagina

during a hysterectomy, extreme care must be taken to differentiate the ureter from the uterine artery - how is this done?
the ureter passes inferior to the artery - “water under the bridge”
the ureter will often “vermiculate” when touched

what 3 layers make up the pelvic floor?
pelvic diaphragm
muscles of perineal pouches
perineal membrane

what two muscle groups make up the pelvic diaphragm?
levator ani and coccygeus

what is the role of the urogenital hiatus?
this is an anterior gap between medial borders which acts as a passage for urethra and vagina

what are the 3 different parts of the levator ani muscle?
puborectalis, pubococcygeus and iliococcygeus

identify the additonal support structures of the pelvic floor?
the endo-pelvic fascia and pelvic ligaments

where is the deep perineal pouch located and what does it contain?
lies below the fascia covering the inferior aspect of the pelvic diaphragm and lies above the perineal membrane
contains part of the urethra (and vagina in females), bulbourethral glands in male, NVB for penis/clitoris, extensions of the ischioanal fat pads and muscles

where is the perineal membrane located and what is its role?
superficial to deep perineal pouch
it is a thin sheet of tough, deep fascia which attaches laterally to the sides of pubic arch, closing the urogenital triangle
it has openings for the urethra (and vagina in females) and togeher with the perineal body, it is the last passive support of the pelvic organs

in the female, what does the superficial perineal pouch (lies below perineal membrane) contain?
contains female erectile tissue and associated muscle
- clitoris and crura = corpus cavernosum
- bulbs of vestibule = paired
- assoc muscles = bulbospongiosis and ischiocavernosus
also contains greater vestibular glands, superficial transverse perineal muscle and branches of internal pudendal vessels and pudendal nerve

what is a vaginal prolapse, how does it present and what are the different kinds?
herniation of urethra, bladder, rectum or rectouterine pouch through supporting fascia
presents as a lump in vaginal wall
kinds = urethrocele, cystocele, rectocele, enterocele

what is a uterine prolapse and how does it present?
descent of uterus
presents = dragging sensation, feeling of “lump”, urinary incontinence
*can be 1st degree, 2nd degree or 3rd degree

how is a vaginal / uterine prolapse repaired and what are the risks of this?
sacrospinosus fixation - sutures placed in sacrospinosus ligament, just medial to ischial spine, to repair cervical / vault descent
this is performed vaginally
risk of injury to pudendal NVB and sciatic nerve

how is urinary incontinence repaired?
trans-obturator approach where there is mesh through obturator canal (space in obturator foramen for passage of obturator NVB) and create a sling around the urethra
incisions through vagina and groin

identify the structures within the lateral pelvic wall?

identify the bones and ligaments within the lateral pelvic wall?

identify the muscles of the lateral pelvic wall?

the majority of the arteries of the pelvis and perineum arise form the internal iliac artery - what are the exceptions?
gonadal artery = arises from L2 abdominal aorta
superior rectal artery = continuation of inferior mesenteric

identify the arteries of the lateral pelvic wall in the male?

identify the arteries of the male perineum?

identify the arteries of the lateral pelvic wall in the female?

what anastomosis occurs in the female pelvis?
between uterine artery and ovarian artery
also between the uterine artery and the vaginal artery

identify the arteries within the female perineum?

where do the venous plexuses of the pelvis mainly drain?
to the internal iliac vein
*some will drain via superior rectal into hepatic portal system
*some will drain via lateral sacral veins into internal vertebral venous plexus

identify the nerves of the lateral wall of the pelvis?
*pudendal nerves supplies majority of perineum

describe the lymphatic drainage of the pelvis?
superior pelvic viscera - external iliac nodes, common iliac, aortic, thoracic duct and venous system
inferior pelvic viscera - deep perineum, internal iliac nodes, common iliac, aortic, thoracic duct and venous system
superficial perineum - superficial inguinal nodes

describe the concept of “trans-peritoneal spread”?
disease can penetrate through the peritoneal layer and disseminate into the peritoneal cavity
