Hemodynamics 1 and 2 Flashcards
Role of the Cardiovascular System (9)
- Move oxygen from the lungs to all body cells
- Move nutrients and water from the gastrointestinal system to all body cells
- Move metabolic wastes from all body cells to kidney for excretion
- Move heat from cells to skin for dissipation
- Move carbon dioxide from body cells to lungs for elimination
- Move particular toxic substances from some cells to liver for processing
- Move hormones from endocrine cells to their targets
- Move stored nutrients from liver and adipose tissue to all cells
- Carries immune cells, antibodies, and clotting proteins to wherever they are needed
Pulmonary vs. Systemic Circulation
- Pulmonary
- Right heart –> lungs
- Permit gas exchange (oxygenation of the blood and removal of CO2)
- Systemic
- Left heart –> body (except lungs)
- Perfuses all the cells of the body
Anatomy of the Cardiovascular System
- Superior and inferior vena cava
- Blood is blue b/c carries less oxygen than blood in systemic circulation
- Right atrium
- Tricuspid valve
- Assures unidirectional blood flow
- Right ventricle
- Pulmonary semilunar valve
- Pulmonary arteries
- Lungs
- Blood is oxygenated
- Pulmonary veins
- Left atrium
- Bicuspid (mitral) valve
- Left ventricle
- Aortic semilunar valve
- Aorta
- Distributes oxygenated blood throughout body
What heart is enclosed in and mainly comprised of
- Heart is enclosed in a tough membranous sac: pericardium
- Heart is mainly comprised of cardiac muscle: myocardium
Matching of Pulmonary and Systemic Blood Flow
- Volume of blood leaving left and right heart per unit time must be matched
- Otherwise, fluid would accumulate in one system
- Ex. Severely damaged left ventricle (congestive heart failure)
- Blood would accumualte in pulmonary circulation
- –> impairment of gas exchange in the lungs
Blood
- Liquid medium: plasma
- 50-55% blood volume
- Contains plasma proteins (albumin, globulin), electrolytes, hormones, enzymes, and blood gases
- Formed elements
-
Red cells (erythrocytes)
- 40-45% total blood volume
- Centrifuged: settle to bottom
- Hematocrit: volume of RBCs in blood
- Contain hemoglobin: bind w/ & transport oxygen
-
White cells (leukocytes)
- 5% total blood volume
- Centrifuged: settle on top of red cells
- For immune processes & bodily defense
-
Platelets
- Little blood volume
- For blood coagulation
-
Red cells (erythrocytes)
Fluid Flow & Pressure
- Fluid moves form regions of higher pressure to regions of loewr pressure
- Contraction of ventricles imparts pressure
- Friction is lost as blood flows through blood vessels

Ohm’s Law
- ( Q = ΔP/R ) or ( ΔP = Q * R ) or ( R = ΔP/Q )
- ΔP = change in pressure on two ends of a vessel (not within the vessel itself)
- Q = blood flow
- R = resistance
- Flow through a vessel will be directly proportional to pressure and inversely proportional to resistance
- Ex. if you increase the length of a vessel, you increase resitance and decrease flow
Poiseuille’s Law
- Q = πΔPr4/ 8ηl
R = 8ηl / πr4- Q = flow
- π/8 is a constant
- ΔP = the pressure driving force
- r = radius of the vessel
- η = viscosity of the fluid
- l = length of the vessel
- Explains the flow of fluid through tubes of different sizes
- A change in radius has a huge effect on blood flow
- If halve the radius, you decrease blood flow by 16x
- Only valid under conditoins of laminar flow
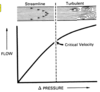
Laminar vs. Turbulence / Tubulent Flow
- Laminar flow
- Fluid on the inside moves faster than the fluid on the outside of a vessel
- Large vessel: fluid flows faster
- Small vessel: fluid flows slower
- Ex. normal blood flow
- Turbulence
- As flow velocity increases, eventually a criticla velocity is reached at which the concentric layers break down
- –> side-to-side motion of fluid
- Increased turbulence –> increased viscosity –> decreased flow
- Turbulent Flow
- Frictional resistance is increased
- The bigger the vessel (increased diameter) and the quicker the blood flow (increased velocity), the more likely turbulent flow will occur
- Sounds which emanate from the circulatory system (murmurs) are the result of localized turbulence
Reynold’s Number (Re)
- Re = dvD/η
- d = fluid density
- v = velocity
- D = tube diameter
- η = viscosity
- Critical Re = 1000
-
Re < 1000 –> laminar flow
- Smaller vessels
- Decreased velocity
-
Re > 1000 –> turbulen flow
- Larger vessels
- Increased velocity
Poiseuille’s Law and Vasodilation/Vasoconstriction
- Can affect blood flow by altering blood vessel size via vasodilation/vasoconstriction
- Vasodilation –> decreased resistance –> increased blood flow
- Vasoconstriction –> increased resistance –> decreased blood flow
Poiseuille’s Law and Hematocrit
- Increased hematocrit –> increased viscosity –> increased resistance –> decreased blood flow
- Anemia: low hematocrit, increased blood flow
- Polycythemia: high hematocrit, decreased blood flow
Blood Pressure: Systole, Diastole, Pulse, Pulse Pressure
- Systole: cardiac muscle contracts
-
Diastole: cardiac muscle relaxes
- Lasts 2x as long as systole
- If heart rate = 67
- Cardiac cycle = 900 ms
- Diastole = 600 ms
- Systole = 300 ms
- Pulse: wave transmitted when the left ventricle contracts
-
Pulse pressure: amplitude of pulse wave
- Depends on the volume of blood ejected and the compliance of the arteries
Blood Pressure: Potential vs. Kinetic Energy
- Arteries contain fibrous and elastic connective tissue
- When high-pressure blood contacts arterial walls, potential energy is absorbed when the artery becomes stretched
- Energy is released as kinetic energy through elastic recoil
- Process limits the drop in arterial pressure during diastole
- Flow of blood from arteries to capillaries is continuous even though the flow from ventricle to aorta is pulsatile

Effect of Gravity on CV Control
- Overcoming gravity: greatest challenge that the CV system faces
- Normal MAP = 100mmHg = column of blood 4.5 ft high
- BP changes
- BP decreases as blood is propelled upward
- BP increases as blood moves down w/ gravity
- When standing
- Arterial pressure at head = 70mmHg
- Arterial pressure at feet = 170mmHg

Dicrotic Notch / Incisura

- Aorta absorbs energy during systole and resorbs it during diastole
- In the left ventricle, when it relaxes, BP drops significantly
- Pressure doesn’t drop as rapidly in the aorta as in the left ventricle
- There’s a brief period at the end of systole when blood flows backwards from the aorta in the ventricle
- Triggers closure of the aortic valve and termination of retrograde flow
- Aortic valve opens when pressure in left ventricle > aorta
- Aortic valve closes when pressure in left ventricle < aorta
- Dicrotic Notch / Incisura: discontinuity in the pressure tracing, marker for aortic valve closing
Pressure Waves in Arterioles
- As arteries divide into smaller branches, the amount of connective tissue in the walls diminishes but muscularity increases
-
Arterioles: major resistance vessels, so BP drops when blood flows through them
- As the pressure wave progresses through them, the pulse is almost completely damped out

Law of Laplace
- Describes surface tension and why large arteries contain more connective tissue than small arteries
- T = Pr
- T = wall surface tension
- P = transmural pressure
- r = radius
- Small vessels can sustain a high pressure w/o having a high surface tension and breaking
- Large vessels need a lot of connective tissue reinforcement to sustain pressure since surface tension is high

How blood flows from arterioles to capillaries to venules
-
Capillaries: single layer of endothelial cells + basement membrane
- Thickness of the wall is only ~0.5 micrometers
- Metarterioles: specialized blood vessels that permit large white cells to flow form the arterial to the venous side of circulation
-
Precapillary sphincters: small bands of vascular smooth muscle at the junciton b/n a metarteriole and a capillary
- When contract, they diminish blood flow into capillaries and shunt blood away from capillary beds

Flow Rate of Materials through Capillaries
- V = Q / A
- V = velocity of blood flow
- Q = flow rate
- A = cross sectional area
- Flow rate through capillaries is lower than arteries veins b/c the toal surface area of capillaries is enormous
- Surface area of capillaries > arteries b/c there are more capillaries than arteries in the CV system

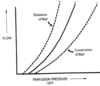
Venous Compliance and its changes with Vascular Smooth Muscle and Aging
- ΔP = ΔV/C
- At higher pressures and volumes, vein compliance decreases and vessels become stiffer (similar to arterial compliance)
- At lower pressures and volumes, compliance is greater, so veins can accommodate a large change in blood volume w/ a small change in pressure
- Vascular smooth muscle
- Contraction –> increased vascular tone –> decreased vascular compliance
- Relaxation –> decreased vascular tone –> increased vascular compliance
- Aging –> increased compliance –> increased blood pooling –> reduced venous return –> orthostatic hypotension

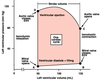
Cardiac Cycle
-
Cardiac cycle: one “pumping cycle” of the heart
- If blocked, ventricles will contract at a different rate than atria
- Pacemaker cells: all elements in conduction pathway
-
Autorhythmic cells: generate action potentials to control cardiac muscle contraction
- Initiation of an AP at one cell –> electrical activity spread throughout heart –> coordinated contraction of atria & ventricles
- Coupled via gap junctions so electrical activity can pass from autorhythmic cells to myocardial cells
- Depolarization
- SA node: in right atrium near superior vena cava, conducts faster
- atria: contract
- AV node: near floor of righ atrium, conducts slowly to ensure ventricles contract after atria
- Bundle of His: conducts rapidly
- ventricles: contract from bottom to top to squeeze blood up to pulmonary artery
- Purkinje fibers: carry impulses from bottom of heart to top

Cardiac Cycle: Mechanical Events
-
Late diastole: atria & ventricles are relaxed, passive ventricular filling
- Atrial pressure > ventricular pressure
- AV valves are open, semilunar valves are closed
- ~80% of ventricular filling occurs during this phase
-
Atrial systole: atrial contraction forces ~20% of additional blood into the ventricles
- End-diastolic volume (EDV): max amount of blood in ventricls at the end of ventricular relaxation (135ml)
-
Isovolumic ventricular contraction: first phase of ventricular contraction pushes AV valves closed but doesn’t create enough pressure to open semilunar valves
- Systole: geneconsidered the time when ventricles contractrally
-
Ventricular ejection: as ventricular pressure rises & exceeds pressure in the arteries, the semilunar valves open & blood is ejected
- End-systolic volume (ESV): minimum amount of blood in ventricles (65ml)
-
Stroke volume: amount of blood ejected during each cardiac cycle (70ml)
- SV = EDV - ESV
-
Ejection fraction (EF): fraction of EDV ejected out of the ventricles during each contraction
- EF = SV/EDV = 70ml / 135ml = 0.52
- Isovolumetric ventricular relaxation: as ventricles relax, pressure in ventricles drops, blood flows back into cups of semilunar valves & snaps them closed

Pressure-Volume Graph
- A: AV valves open
- AV valve opens when atrial pressure > ventricular pressure
- Ventricular diastole: ventricles fill
- Ventricular pressure increases slightly as volume increases
- Atria contract, & ventricles contain the max amount of blood
- End-diastolic volume (EDV) = 175ml
- B: AV valves close
- AV valve closes when ventricular pressure > atrial pressure
- Ventricles begin to contract
- Isovolumetric contraction: ventricular pressure increases as volume stays constant
- C: Semilunar valves open
- When semilunar valves open, blood is ejected into the aorta & pulmonary arteries
- Ventriuclar pressure continues to increase as ventricular volume drops
- Ventricles begin to relax, & semilunar valves close
- End-systolic volume (ESV) = 65ml
- D: Semilunar valves close
- isovolumetric relaxation: pressure drops as volume remains the same
- AV valves remain closed b/c ventricular pressure > atrial pressure
- When ventricular pressure drops below atrial pressure, AV valves open
ECG
- P wave: atrial depolarization
- QRS waves: ventricular depolarization (& atrial repolarization)
- T wave: ventricular repolarization
- RR interval: heart rate

Wiggers Diagram

- a wave: atrial contraction
-
c wave: ventricular contraction due to…
- Backflow of blood from ventricle to atrium when mitral valve closes
- Bulging of the closed mitral valve backward into the atrium when ventricular pressure increases
- v wave: blood flowing from the veins into the atrium during ventricular contraction
