A. TSH < 0.01, Free T3 15.6, Free T4 38.0.
- Consistent with clinical primary hypothyroidism
- 2.Consistent with euthyroid status in a patient complaining of tiredness.
- 3.Consistent with pituitary driven thyrotoxicosis
- 4.Consistent with secondary or pituitary hypothyroidism.
- 5.Consistent with sub-clinical hypothyroidism with risk of later clinical hypothyroidism.
- 6.Consistent with thyrotoxicosis.
- 7.To screen for medullary thyroid carcinoma
- 8.To screen for recurrence of differentiated thyroid carcinoma.
Normal ranges TSH 0.33-4.5mU/L Free T3 (3.2-6.5pmol/L) Free T4 (10.2-22.0pmol/L) Thyroglobulin <5 ug/L
6
TSH 8.4, Free T4 11.7, Thyroid peroxidase (thyroid antibodies) positive
- Consistent with clinical primary hypothyroidism
- 2.Consistent with euthyroid status in a patient complaining of tiredness.
- 3.Consistent with pituitary driven thyrotoxicosis
- 4.Consistent with secondary or pituitary hypothyroidism.
- 5.Consistent with sub-clinical hypothyroidism with risk of later clinical hypothyroidism.
- 6.Consistent with thyrotoxicosis.
- 7.To screen for medullary thyroid carcinoma
- 8.To screen for recurrence of differentiated thyroid carcinoma.
Normal ranges TSH 0.33-4.5mU/L Free T3 (3.2-6.5pmol/L) Free T4 (10.2-22.0pmol/L) Thyroglobulin <5 ug/L
5
TSH 1.4, Free T4 12.1.
- Consistent with clinical primary hypothyroidism
- 2.Consistent with euthyroid status in a patient complaining of tiredness.
- 3.Consistent with pituitary driven thyrotoxicosis
- 4.Consistent with secondary or pituitary hypothyroidism.
- 5.Consistent with sub-clinical hypothyroidism with risk of later clinical hypothyroidism.
- 6.Consistent with thyrotoxicosis.
- 7.To screen for medullary thyroid carcinoma
- 8.To screen for recurrence of differentiated thyroid carcinoma.
Normal ranges TSH 0.33-4.5mU/L Free T3 (3.2-6.5pmol/L) Free T4 (10.2-22.0pmol/L) Thyroglobulin <5 ug/L
2
TSH 22. 4, Free T4 6.3.
- Consistent with clinical primary hypothyroidism
- 2.Consistent with euthyroid status in a patient complaining of tiredness.
- 3.Consistent with pituitary driven thyrotoxicosis
- 4.Consistent with secondary or pituitary hypothyroidism.
- 5.Consistent with sub-clinical hypothyroidism with risk of later clinical hypothyroidism.
- 6.Consistent with thyrotoxicosis.
- 7.To screen for medullary thyroid carcinoma
- 8.To screen for recurrence of differentiated thyroid carcinoma.
Normal ranges TSH 0.33-4.5mU/L Free T3 (3.2-6.5pmol/L) Free T4 (10.2-22.0pmol/L) Thyroglobulin <5 ug/L
1
Thyroglobulin 254
- Consistent with clinical primary hypothyroidism
- 2.Consistent with euthyroid status in a patient complaining of tiredness.
- 3.Consistent with pituitary driven thyrotoxicosis
- 4.Consistent with secondary or pituitary hypothyroidism.
- 5.Consistent with sub-clinical hypothyroidism with risk of later clinical hypothyroidism.
- 6.Consistent with thyrotoxicosis.
- 7.To screen for medullary thyroid carcinoma
- 8.To screen for recurrence of differentiated thyroid carcinoma.
Normal ranges TSH 0.33-4.5mU/L Free T3 (3.2-6.5pmol/L) Free T4 (10.2-22.0pmol/L) Thyroglobulin <5 ug/L
8
What naturally occurring compound blocks TSH?
Perchlorate
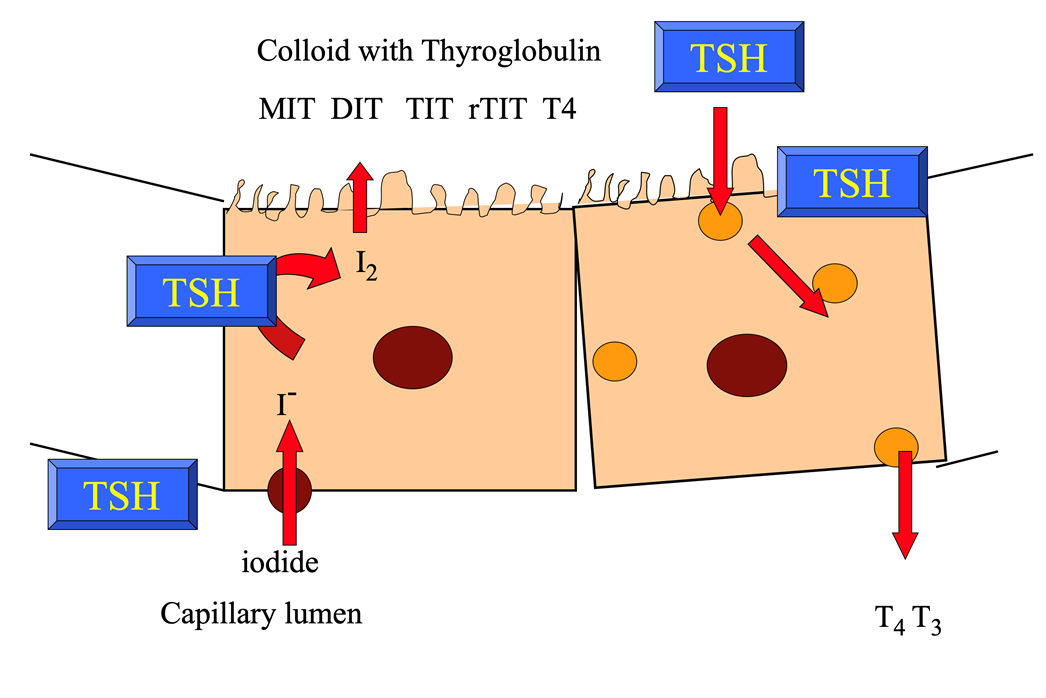
Describe the molecular mechanisms of T3/4 production.
This occurs in thyrocytes in thyroid follicles.
- Iodide goes through the membrane via Na+/K+ ATPase
- Iodide –> iodine by thyroid peroxidase (TPO)
- The iodine is then taken up by thyroglobulin(TG) and –> thyroxine through a number of processes involving TPO –>MIT and TIT via iodination of tyrosine residues in thyroglobulin
- There is coupling of monoiodotyrosine (MIT) and DIT to form T3 and 2 diiodotyrosine (DIT) to form T4
- Once the thyroxine (T4) is produced, it is stored within the thyroid gland (and taken up by BM again and secreted into the lumen when required)
- In the periphery, T4 –> T3
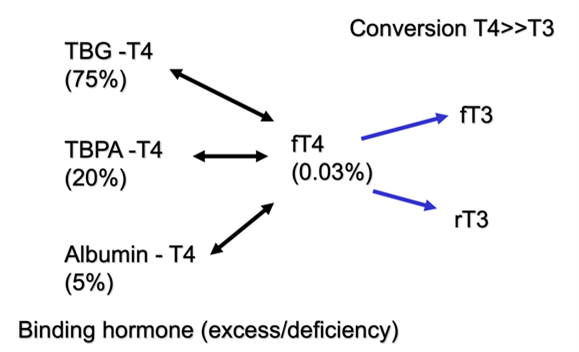
Which form is thyroxine most commonly found in the periphery?
- A very small proportion is active thyroxine (fT4)
- Only 0.03% of thyroxine in the circulation is active
- Thyroxine can bind to thyroxine-binding pre-albumin (TBPA) & albumin
- Most of the thyroxine is bound to thyroxine binding globulin (TBG) – 75%
- NOTE: if lacking albumin in diet, you TBG levels will go down
Describ the axis.
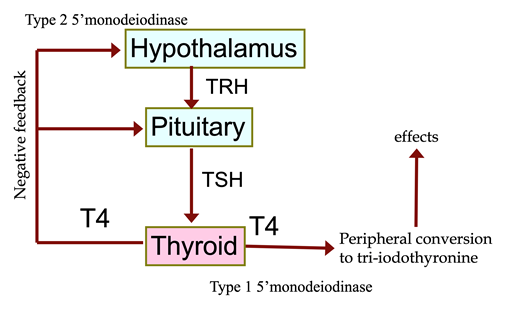
- Hypothalamus produces TRH à stimulates production of TSH from pituitary gland à stimulates T4 production
- T4 converted to T3 in peripheries (active component of thyroxine)
- Too much T4 –> feedback to the hypothalamus to prevent it from producing too much TRH
- So, if you have low T4, you should have high TRH and high TSH
NB: hCG and TSH have similar structures (hCG has 1/10,000 activity of TSH) and so can stimulate same actions I.E. a string around the neck is used as a pregnancy test in Africa (hCG –> goitre)
List the most common causes of hypothyroidism.
Most hypothyroidism is PRIMARY
- Hashimoto’s thyroiditis (autoimmune)
- Atrophic thyroid (congenital or age)
- Post-Graves’ disease (radioactive iodine, surgery, natural history or thionamines)
- Other minor causes:
- Post-thyroiditis
- Drugs (amiodarone, lithium)
- Thyroid agenesis or dysgenesis
- Iodine deficiency and dyshormonogenesis
- 2nd hypothyroidism (pituitary disease)
- Peripheral thyroid hormone resistance
What are the clinical features of hypothyroidism?
- Metabolic rate - reduced –> weight gain
- Cardiovascular - bradycardia
- Gastrointestinal - constipation
- Respiratory- laboured breathing
- Reproductive - oligomenorrhoea
- Other:
- Weight gain (metabolic rate issues) and poor appetite
- Cold/dry hands/feet
- Hyponatraemia (thyroxine is involved with Na transport in kidneys)
- Normocytic anaemia + pernicious anaemia)
- Myxoedema, goitre
- Subtle in the elderly
What investigations should be done for primary hypothyroidism? What other conditions should you test for?
- High TSH + Low T4 if primary
- Thyroid peroxidase autoantibodies (suggests autoimmune hypothyroidism / Hashimoto’s thyroiditis)
- Remember to consider any other autoimmune conditions that the patient may also have (e.g.
- pernicious anaemia
- coeliac disease
- Addison’s disease
What is the management of primary hypothyroidism?
- Perform an ECG:
- If there is co-cardiac failure alongside the hypothyroidism, giving levothyroxine will exacerbate any myocardial ischaemia and MAY worsen the heart failure à start at a VERY low dose and titrate
- Levothyroxine (T4), 50-125-200 mcg/day -
- Titrated to a normal TSH
- Titrated by BMI, most patients are on about 100mcg,
- Liothyronine (T3)
What is the problem with overtreating patients with T4? Is there evidence for T3 rather than T4?
- NO evidence base for over-treating patients with too much T4
- Some patients prefer to take too much thyroxine because it helps them lose weight
- Excessive thyroxine can cause osteopaenia and AF
- There is NO evidence base for giving T3 rather than T4
- T4 is sometimes converted to T3 in some tissues; patients think that T3 is more natural.
What type of hypothyroidism is associated with normal T4 but high TSH?
Subclinical hypothyroidism (SH) / “Compensated Hypothyroidism”
- T4 level is NORMAL but TSH is HIGH
- Pituitary gland senses T4 and* thinks the thyroid is NOT producing enough thyroxine so it produces more TSH
Which antibody if positive in subclinical hypothyroidism, may indicate thyroid disease?
If TPO antibodies are positive, it suggests that may –> thyroid disease
Is there any benefit of treating subclinical hypothyroidism? Does it help with symptoms?
Generally asymptomatic
Subclinical hypothyroidism is UNLIKELY to be the cause of their presenting symptoms – no change in symptoms will occur.
But hypothyroidism is associated with hypercholesterolaemia (may be only benefit of treating SH)
How soon after radioiodine treatment do patients become hypothyroid?
Usually hypothyroid within 1 year of receiving treatment
But may take many years in some patients (up to 15yrs) ( 50% of patients)
Describe the changes in thyroid function in pregnancy and why they occur.
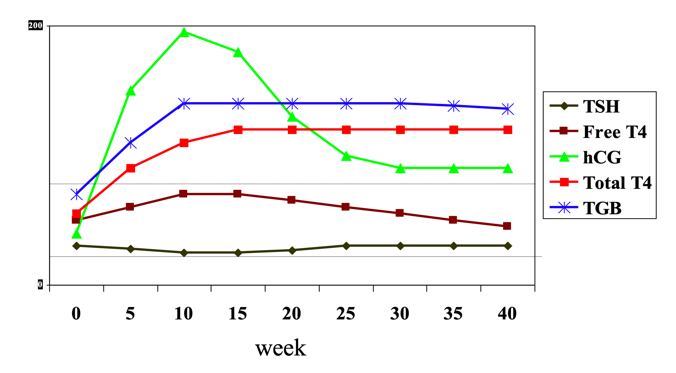
- hCG has a similar structure to TSH - so can bind onto THSr and cause thyroid to produce more thyroxine
- Can cause thyrotoxicity if malignancy produces hCG
- Rise in hCG in the 1st trimester –> increase in free T4 but this is a normal physiological process
- Normal ranges’ of TSH and T4 in pregnancy are slightly different to non-pregnancy
- Later in pregnancy, hCG levels will drop –> T4 levels drop and TSH levels will rise slightly
- TBG levels increase in pregnancy (as TBG is under the control of oestrogen) – but cannot be measured in serum, only T4
If T4 was low or extremely high at the start of pregnancy then this would be abnormal.
What is the most thing to remember when testing for neonatal hypothyroidism?
Test must be done at the appropriate time (48-72hrs) after birth otherwise you may be detecting the mother’s TSH and miss the neonatal hypothyroidism (common as occurs in 1 in 3500)
Done using Guthrie test
What is sick euthyroid syndorme? How is it managed?
Occurs when severe illness affects the HPT axis and thyroid may shut down to reduce the BMR BUT no hypothyroid symptoms occur and no improvement on giving thyroxine
- Biochemistry
- Low T4 and T3 (and reduced T3 action)
- Normal/high TSH (later decreased)
What are the causes of hyperthyroidism and how can they be divided?
High uptake and low uptake on technetium scan
- HIGH UPTAKE:
- Graves’ disease- 40-60%
- Toxic multinodular goitre - 30-50%
- Single toxic adenoma - 5%
- LOW UPTAKE:
- Sub-acute thyroiditis / viral thyroiditis / de Quervain’s thyroiditis (all the same)
- Postpartum thyroiditis
Rare causes:
- Silent thyroiditis (AI, amiodarone)
- Factitious thyroiditis
- TSH-induced
- Thyroid cancer induced
- Trophoblastic tumour and Struma ovarii (high hCG production)
List 2 causes of low and high uptake on technetium scan.
Technetium scan can be used to see which parts of the thyroid are producing excessive thyroid hormone. All three of the above conditions that are high uptake will show increased uptake of technetium
- Graves’ disease
- Toxic multinodular goitre
- Single toxic adenoma
In pregnancy, the body may produce antibodies that stimulate the thyroid gland to release excess amounts of thyroxine. These have low uptake in a technetium scan:
- Postpartum thyroiditis
- Sub-acute thyroiditis, de Quervain’s
What are the clinical features of hyperthyroidism?
- Metabolic rate- increased –> weight loss
- Cardiovascular - tachycardia
- Gastrointestinal- diarrhoea
- Respiratory - tachypnoea
- Skeletal - osteopaenia & osteoporosis (thyroxine acts on osteoclasts)
- Reproductive - irregular periods




-
CHEMPATH: Lipids Lecture47
-
CHEMPATH: LFTs and cases37
-
CHEMPATH: Clinical chemistry CPC46
-
CHEMPATH: Calcium Handling54
-
CHEMPATH: Sodium and Fluid Balance39
-
CHEMPATH: Potassium Handling34
-
CHEMPATH: Acid-base handling27
-
CHEMPATH: Diabetes cases24
-
CHEMPATH: Diabetes CPC17
-
CHEMPATH: Hypoglycaemia47
-
CHEMPATH: Adrenal Disease21
-
CHEMPATH: Pituitary31
-
CHEMPATH: Thyroid39
-
CHEMPATH: Porphyrias42
-
CHEMPATH: Acute kidney injury and chronic kidney disease47
-
CHEMPATH: Assessment of renal function35
-
CHEMPATH: Uric acid metabolism31
-
CHEMPATH: Metabolic disorders and screening (1+2)68
-
CHEMPATH: Paediatric clinical chemistry38
-
CHEMPATH: Nutrition43
-
CHEMPATH: EMQs on enzymes and chemistry32
-
CHEMPATH: Enzymes and Cardiac Markers21
-
HISTO: Liver CPC74
-
HISTO: Fundamentals of Histology35
-
HISTO: Lung pathology77
-
HISTO: Skin Pathology41
-
HISTO: Breast54
-
HISTO: Systemic Pathology29
-
HISTOPATH: Neuro-oncology66
-
HISTO: Upper GI pathology59
-
HISTO: Lower GI Disease44
-
HISTO: Neuropathology50
-
HISTO: Gynaecological Pathology104
-
HISTO: Neurodegeneration54
-
HISTO: Endocrine disease79
-
HISTO: Cardiovascular89
-
HISTO: Pancreas and gallbladder52
-
HISTO: Urological pathology85
-
HISTO: Immune related multisystem disorders – Connective tissue disease, amyloid, sarcoid50
-
HISTO: Liver pathology53
-
HISTO: Renal pathology70
-
HISTO: Bone Tumours67
-
HAEM: Coagulation65
-
HAEM: Venous Thrombosis45
-
HAEM: Haemolytic anaemias38
-
HAEM: Systemic disease53
-
HAEM: Multiple myeloma, amyloid and MGUS45
-
HAEM: Blood transfusion89
-
HAEM: Lymphoma: MDT, CLL, NHL, lymphoproliferative disorder87
-
HAEM: Acute leukaemia53
-
HAEM: Myeloproliferative disorders53
-
HAEM: CML and MPD (polycythaemia)66
-
HAEM: Myelodysplastic syndromes/ Bone marrow failure61
-
HAEM: Bone marrow transplant42
-
HAEM: Paediatric haematology51
-
HAEM: Obstetric haematology59
-
HAEM: Interactive cases0
-
MICRO: Antimicrobials 184
-
MICRO: Antimicrobials 244
-
MICRO: Healthcare associated infections28
-
MICRO: CNS infections and meningitis44
-
MICRO: Fungal infections46
-
MICRO: Vaccines25
-
MICRO: Mycobacterial diseases (TB)46
-
MICRO: Wound, Bone and Joint Infections37
-
MICRO: Zoonoses44
-
MICRO: GI infections78
-
MICRO: Prion disease44
-
MICRO: Respiratory tract infections66
-
MICRO: HIV in African children25
-
MICRO: Urinary Tract Infections45
-
MICRO: Opportunistic viral infections51
-
MICRO: Infection CPC39
-
MICRO: Viral hepatitis72
-
MICRO: ‘21st century pandemics: influenza and COVID’33
-
MICRO: Antivirals68
-
MICRO: Neonatal and childhood infections51
-
IMMUNO: Autoimmune and Autoinflammatory Disease120
-
IMMUNO: Transplantation42
-
IMMUNO: Immune response to infection73
-
IMMUNO: Primary Immunodeficiency100
-
IMMUNO: Immune modulating therapies120
-
IMMUNO: Allergy38
-
IMMUNO: Secondary immune deficiencies and HIV infection52
-
TBL sessions0
-
ETHICS: Human Rights and Global Justice28
-
MICRO: Fever in the returning traveller34
-
MICRO: Global health priorities and brain worms23
-
MICRO: Tuberculosis and Development6
