Facial Aging & Rhytidectomy Flashcards
What are the five anatomical layers of the face
- Skin: firmly attached to the underlying SC w cutis retinacula
- Subcutaneous/Superficial fat compartments (5)
- Nasolabial
- Medial Cheek
- Middle Cheek
- Lateraltemporoparietal (cheek)
- Inferior orbital
- Superficial musculoaponeurotic System
- = superficial fascia and mimetic muscle
- continuous w plastysma (superficial cervical) fascia, TPF, galea
- Fixed over the parotid, mobile medial to parotid and fuses again medially at NLF
- Parotidomasseteric fascia - Deep facial fascia
- continuous w superficial leaflet of DTF, into neck as deep cervical fascia
- Neurovascular structures are in and deep to PM fascia
- Bone/periosteum

Name the muscles in the face (4 layers)
- Zm, Oo, DAO
- Risorius, Plastysma, DLI
- ZM, LLSAN, LLS, Ooris
- Mentalis, LAO, Buccinator * innervated on superficial surface
+ procerus
+ depressor supercilli
LLSAN, LLS, Zn, ZM (from medial to lateral)
Mentalis, DLI, DAO (from medial to lateral)
What is the blood supply to the face and main branches
- central
- middle
- outer/lateral
- scalp/forehead
External carotid
Internal carotid (ophthalmic artery ->eyebrow, lid, forehead, scalp)
- Central: angular, Nasal, S&I labial,
- Middle: facial, M&P jugular, submental, infraorbital
- Lateral: S&I masseteric, transverse facial, Zygomatico-orbital
- Scalp forehead: STA, SO, post auric, occipital
Describe the course of the facial branches
-
Frontal
- Course; 0.5cm below tragus to 1.5cm above lat brow (pitangays line). AT midpoint b/w tragus and lat canthus, nerve crosses arch
- Inf to arch: deep to PM
- At arch, on periosteum+sup.leaf of DTF
- Sup to arch, deep to TPF
-
Zygomatic
- deep to PM, above masseter
- VULNERABLE at anterosuperior parotid, deep to orgin of Z.M at 3cm anterior to tragus
-
Buccal
- vulnerable at anterior parotid, deep to PM
-
Marginal Mandibular
- exits anteroinferior parotid - deep to PM, deep cervical fascia
- always deep to plastysma, protected by deep cervical fascia
- posterior to facial vessels, nerve lies inferior to mandible
- anterior to facial vessels, nerve lies superior to mandible
-
Cervical
- penetrates deep cervical fascia, runs deep to plastyma at a pint 1/2 b/w mastoid/mentum at angle of manidble

Describe the course of CN11
- exits jugular foramen
- runs along posterior deep surface of SCM
- leaves posterior SCM 7-9cm above clavicle to travel on deep surface of trapezius
What si the anaotmic landmark for he Greater auricular nerve and what is the consequence of its injury
- 6.5cm below EAC, ont he superficial surface of SCM, traveling form posterior to anteriro to course with the EJV
- injury results in numbness of loule, inferior auricular region
What provides the sensory innervation to the face
- external nasal
- infratrochlear
- supratrocheal
- supraorbital
- infraorbital
- zygomaticofacial
- zygomaticotemporal
- mental
- buccal
- auriculotemrpoal
- GAN
- LON
- GON

What are the 7 facial danger zones
- GAN : 6.5 cm below EAC
- posterior to SMAS
- =>numbness inferior 2/3 rd of ear, cheek, neck
- Temporal: 0.5cm below tragus to 1.5cm above lat brown
- deep to SMAS
- =>paralysis of frontalis
- Marginal mandibular: 2cm posterior to oral comissure, midmanidble
- deep to SMAS (platysma)
- =>paralysis lower lip
- Zygomatic+Buccal : triangle formed by points on malar, oral commisure, posterior angle mandible
- deep to SMAS
- =>paralysis upper lip cheek
- Supraorb/supratroch: SOR at midpupil
- anterior to SMAS
- =>numbness forehead, nose, scalp, upper eyelid
- Infraorbital: 1cm below IOR at midpupil
- anterior to SMAS
- =>numbness side of nose, upper lip, lower eyelid
- Mental: midmandible bwlow 2nd premolar
- anterior to SMAS
- =>numbness to half lower lip/chin
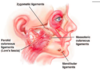
Name the facial retaining ligaments of the face (furnas,stuzin)
Osteocutaneous (Direct)
-
Zygomatic RL*
- along arch/body, posterior to Zm, 4.5cm ant to tragus
- suspends malar fat pad
- deep to ZRL is zyg/buccal branches, parotid duct, trasnverse facial artery
-
Mandibular RL*
- along parasymphysys and anterior 1/3 of body
- posterior limit of MRL defines anterior border of jowl
Indirect cutaneous (between deep and superficial fascia)
- Parotid-preauricular CL (Lore’s fascia)
- Parotid-Masseteric CL*
- Superior temporal line CL
- Platysma CL
- orbicularis RL (orbitomalar ligament)
WHat is contained in the buccal fat pad
- Zygomatic, buccal branches superficial
- parotid duct
What is macgregors patch?
Malar fat pad
= 3 superficial fat compartments
= Nasolabial, medial cheek, inferior orbital
- descends with age and deflates
= deepened NFL and jowls
Describe facial aging by decade and by structure
30s - eyelid, crow feet
40s - NLF, glabella, forehead
50s - neck, jaw, jowls, nasal tip
60s- deepened wrinkles and sagging
Skin: thining epidermis, atrophic dermis, less collagen 1
Soft Tissue - deflation, descend, deterioration
- Middle 1/3 NL and mrionette groove
- Lower 1/3 jowl, witchs chin
Bone - retrusion of IOR and maxilla anteriorly and height
What are rhytids and examples of each type
Creases in the skin due to intrinsic changes in skin structure and perpendicular to muscle movement
- Dynamic - animation creease
- Static fine - disrupted elastin network
- Static coarse - deep caused by solar elastosis
What changes occurs histologically to skin with aging
- Loss of cells
- melanocytes
- langerhans
- Loss of structure
- DE papillae
- reticular dermis
- Loss of substances
- ground substance
- elastin
- collagen type 1 (more t3:t1)
- increase size of sebaceous glands
What changes occur with photoaging
- telangiectasia
- dyschromias:hypo/hyperpigment
- atrophy
- erythema
- static rhytids: fine and deep