How does anesthesia affect ventilation?
- Alter sensitivity to CO2
- Relax respiratory muscles (FRC decreases)
- Atelectasis develops
- Makes V/Q mismatch worse
How does ventilation affect anesthesia?
- Utake of inhalational anesthetics depends on ventilation
- Controlled ventilation facilitates reliable uptake and smooth plane of anesthesia
Ventilation–what is it? What is it defined by (and what is the normal value)? How is it monitored?
- Process involved in the movement of air (gas) in and out of alveoli
- Defined by PaCO2 (inversely proportional)
- Normal PaCO2 ~ 35-45 mmHg
- Monitored with arterial blood gas (PaCO2) or capnography
What is oxygenation? What is it defined by? What is considered hypoxemic (#’s)? How is oxygenation measured?
- Process of oxygenation of arterial blood
- Defined by PaO2
- Hypoxemia
- PaO2 < 60 mmHg
- SaO2 < 90%
- Monitored with arterial blood gas (PaO2) or pulse oximetry
How can oxygenation improve while breathing 100% oxygen? Is apneic oxygenation possible?
- Cannot be improved by more ventilation
- Can be improved by special respiratory maneuvers
- Apneic oxygenation is possible (ventilation may not be needed for oxygenation)
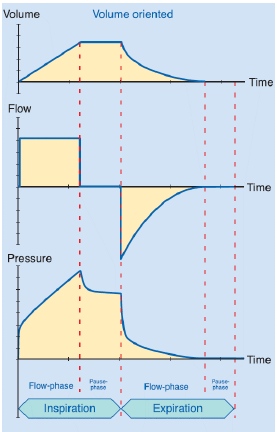
What are the phases of respiration?
- Inspiration
- Inspiratory flow time
- Insiratory pause
- Expiration
- Expiratory flow time
- Expiratory pause
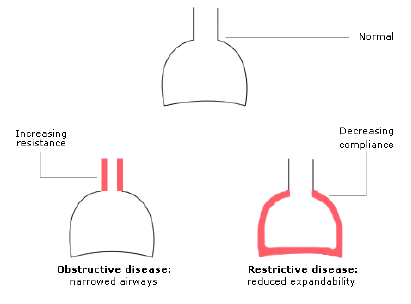
What do resistance and compliance limit?
- Resistance limits flow
- = change in pressure / flow
- Compliance limits volume
- = volume / flow
Indications for mechanical ventilation (MV)?
- There is a need to decrease PaCO2
- #1 indication under anesthesia
- There is a need to increase PaO2
- It’s easier to provide high FiO2 if patient is intubated and breathing 100% O2
- If patient is already intubated and breathing 100% O2 increasing oxygenation will only be possible with special respiratory maneuvers and not with conventional ventilation
- There is a need to decrease respiratory effort
- Mostly happens in ICU as treatment for resp failure
What are the indications for MV during anesthesia (10)?
- Conventional control of resp function
- Prolonged anesthesia
- Maintain more stable anesthesia plane
- Neuromuscular blockade
- Thoracic surgery
- Chest wall or diaphragmatic trauma
- Obesity, inc. abdominal pressure
- Head down positioning (Trendellenburg)
- Laparoscopy
- Control of intracranial pressure
What are the indications for MV in the ICU (6)?
- Depression of resp center in the brain
- Inadequate thoracic expansion
- Inadequate lung expansion
- Obstructed airway
- Resp arrest (or cardio pulmonary arrest)
- Pulmonary edema, ARDS
What are some side effects of MV? What is the treatment?
- Impairs venous return and CO
- May cause hypotension, especially in hypovolemic patients
- Pneumothorax, lung injury
- Treatment
- Volume loading
- Decreasing airway pressures (change ventilator settings)
- Switch off the ventilator
- Inotropic drugs (i.e. dobutamine)
What are the side effects of hypercapnia (direct, indirect, narcosis)?
- Direct effects of CO2
- Peripheral vasodilation
- Decreased myocardial contractility
- Bradycardia, poss. cardiac arrest (very extreme case)
- Increased intracranial pressure
- Indirect effects via catecholamine release
- Tachycardia, arrhythmias
- Increased myocardial contractility
- Increased BP
- CO2 narcosis
- > 95 mmHg progressive narcosis
- > 245 mmHg complete narcosis
What is the risk of not ventilating properly?
If you don’t control ventilation during thoracic surgery and let the lung be collapsed for a prolonged time, not only will CO2 accumulate but the patient will quickly turn hypoxemic and you may encounter sudden death of the patient
Should I ventilate during anesthesia?
- Debated issue, esp. in horses
- Point is how to balance between either comprimising cardiovascular or resp function (and oxygenation)
- Permissive hypercapnia may be acceptable up to 60-70 mmHg
What are the 3 types of ventilation?
- Spontaneous
- Patient determines when and how
- Assisted
- Patient determines when and ventilator determines how
- Mandatory (or controlled)
- Ventilator determines when and how
What are the 2 different ventilation modes?
- Volume controlled
- Device sets the volume, pressure is a dependent variable
- If compliance decreases (pneumothorax), pressure would increase
- Difficult to control the tidal volume in very small patients
- Pressure controlled
- Device sets the pressure, volume is a dependent variable
- If resistance increases (airway obstruction), volume would decrease
- Works well regardless of body size
What are the clinical recommendations for using pressure or volume controlled ventilation?
- If lung volume changes during procedure (e.g. thoracotomy), use pressure controlled ventilation
- If trans-pulmonary pressure changes (e.g. laparoscopy), use volume controlled ventilation
What are the 5 classifications of ventilators?
- Source of driving power
- Control variable
- Cycle variable
- Trigger variable
- Limit variable
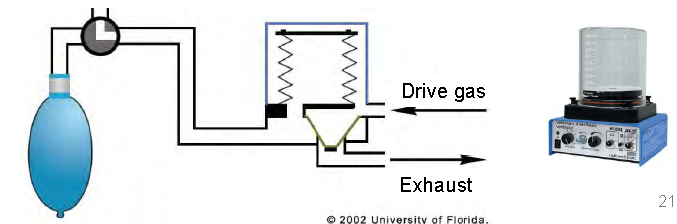
What are the 2 sources of driving power for ventilators?
- Electrically driven (i.e. using a linear motor)
- Pneumatically driven: using pressurized gas source (more common)
Control variable ventilators
- Flow–ventilator delivers constant flow to the patient
- Pressure–ventilator delivers constant pressure to the patient
- Analogy with electricity: Flow is current, pressure is voltage. A battery may supply either constant current or constant voltage
Cycle variable ventilators
- Triggers expiration when set value is reached
- Volume: volume controlled ventilation
- Pressure: pressure controlled
- Time: both
- Flow: diminishing flow triggers expiration
- Useful for pressure support ventilation (PSV) because it helps accommodating to the patients breathing pattern
Trigger variable ventilation
- Triggers inspiration when set value is reached
- Used during assisted ventilation modes
- Pressure: negative pressure triggers a breath
- Flow: inspiratory flow is a trigger.
- Better, more sensitive method
Limit variable ventilation
- When value is reached inspiration will be terminated
- Volume limit: e.g. metal rod limits the expansion of the bellows
- Used in the North American Draeger
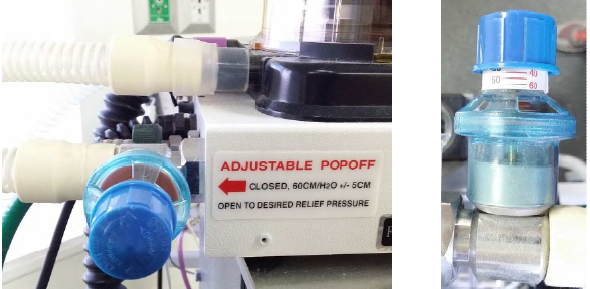
- Pressure limit is used to prevent barotrauma as a consequence of inappropriate ventilator setting
Pressure limiting valve
- Safety pressure limit for the drive gas pressure
- The patient will receive less pressure than this
- RUSVM: set at 20



-
Intro15
-
Machine46
-
Breathing systems52
-
Inhalant anesthesia68
-
Patient evaluation45
-
Principles of monitoring44
-
Monitoring the anesthetized patient37
-
Premedication70
-
Induction24
-
Injectable anesthetics15
-
Blood gas analysis34
-
Recovery38
-
Mechanical ventilation37
-
Neuromuscular blocking drugs21
-
Ruminant anesthesia52
-
Swine anesthesia36
