What considerations exist for eyes with silicone oil having cataract surgery
Never use silicone IOL (debris will accumulate on the lens) Don’t use a tranditional A scan (Ultrasound moves slower in S.O. so the A scan reads longer and will say you need a low powered lens when in fact you need to add power.) Use IOL master (which uses partial coherence infreometry. Adjustments to intraocular lens power: If the silicone oil is to remain in the eye for an extended period of time after cataract surgery, an adjustment to intraocular lens power must be made. Holladay, and others, have recommended that biconvex intraocular lenses should not be placed in patients who have silicone oil in the vitreous cavity. Instead, these patients should have a PMMA convex-plano lens, with the plano side oriented so it is facing towards the vitreous cavity and preferably over an intact posterior capsule. This approach prevents the silicone oil from altering the refractive power of the posterior surface of the intraocular lens. By contrast, a +20.00 diopter biconvex intraocular lens could loose between a third and half of its refractive power if it comes into contact with silicone oil. PMMA lenses are a first choice, and silicone lenses should be avoided. The Holladay IOL Consultant is very helpful for these cases as it is able to automatically compensate for the higher index of refraction of silicone oil in the vitreous cavity when doing these special IOL power calculations. The additional power that must be added to the original IOL calculation for a convex-plano IOL (with the plano side facing towards the vitreous cavity) is determined by the following relationship, as described in 1995 by Patel and confirmed by Meldrum: Ns = refractive index of silicone oil (1.4034). Nv = refractive index of vitreous (1.336). AL = axial length in mm. ACD = anterior chamber depth in mm. Additional IOL power (diopters) = ((Ns - Nv) / (AL - ACD)) x 1,000 For an eye of average dimensions, and with the vitreous cavity filled with silicone oil, the additional power needed for a convex-plano PMMA intraocular lens is typically between +3.0 D to +3.5 D.
How does a keratometer work?
1) a light source illuminates the mires and the cornea acts as a convex mirror creating an image of the mires that is virtual, erect and minified - this is the new object. (you need to derive the size of this image).
2) the object rays then pass through a four apature disk. (two of the holes are a Schenier disk - which just doubles/creates 2 images in anything but perfect focus. Two of the holes are prisms oriented hotizontally and vertically.
3) The machine is rotated to line up the + /-components along the principal meridians, and then the images are focused so the image size is determined.

How does a Direct Ophthalmoscope work.
Bright light source is directed into the pupil via mirror.
Magnification is via simple magnifier and depends on eye error. Power of the eye/4. In an emmetropic eye this is assumed to be 60D so 60/4=15x magnification.
How does the indirect ophthalmoscope work?
It utilizes similar principles to the direct but adds an obective lense (which acts as a condensing lense forming a virtual inverted and magnified view of the object - which is the retina)
M= -60D (of the eye)/+20D (of the condesing lens) = 3x magnified
How does ultrasound work?
Piezoelectric effect - a mechanical stress can be converted to electrical enercy and vise versa. A crystal pulsed with electricity will transduce sound waves. The frequency is too high to be heard. If you raise the energy high enough you get fragmentation (like phaco) or at low energy you get ultrasound where the time delay between emmision and detection is a function of the distance travelled and the density of the substance it travelled through. The denser the medium the faster the travel *recall Silicone oil - floats on water, is less dense so ultrasound moves slower through it - which elongates your A-Scan.
How does the Goldman aplanation tonometer work?
At an applanation of 3.06mm the force required to deform the cornea is cancelled by the surface tension of the tear film so the force applied to the cornea by the tonometer reflects the intraocular pressure (when multiplied by 10.
A spilt prism and vernier acuity to line up the mires is used to determine when 3.06mm of aplanation has been achieved.
LASER - define and describe
Light Amplification by Stimulated Emission of Radiation.
Photons of energy are relaesed from an atom in a coherent fashion by the exitation of electons in orbit around the atom. They are all of the same wavelength (monochromatic) and are amplified by a resonance chamber (constructed in multiples of 1/2 wavelengths so that when they bounce of a mirror they remain coherent and are eventually directed out an aperture at high intensity.
Describe different types of lasers
Gas discharge (argon, krypton, CO2 and eximer) can be exited by the electrons travelling in an electric current between two electrodes.
Semi-conductor lasers (diode), use electrical power to exite electons.
Solid state laser (Nd: Ytridium-aluminum-garnet) use incoherent light from xenon arc flashes to excite the electrons.
Snell’s Law
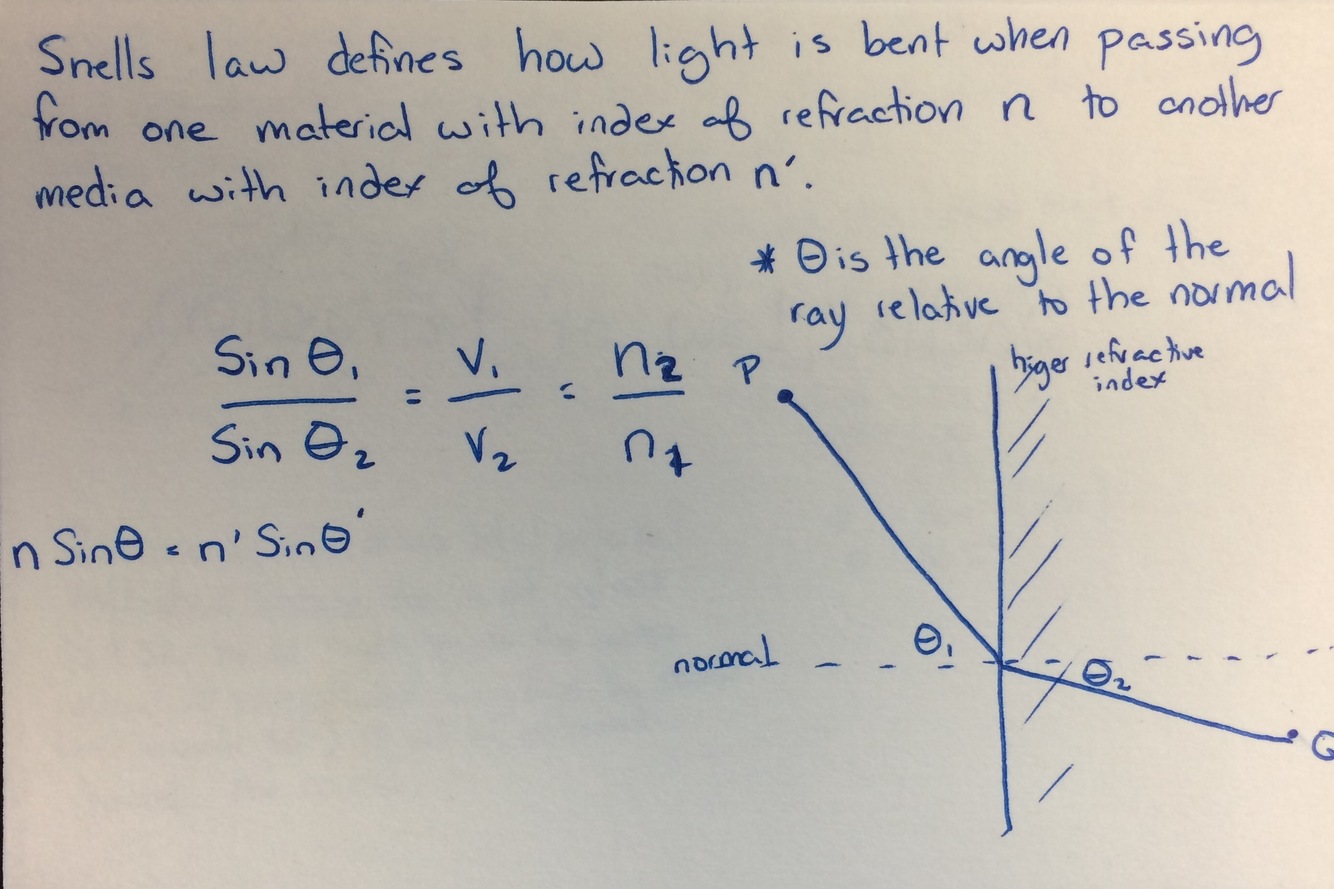
Critical Angle & Total Internal reflection
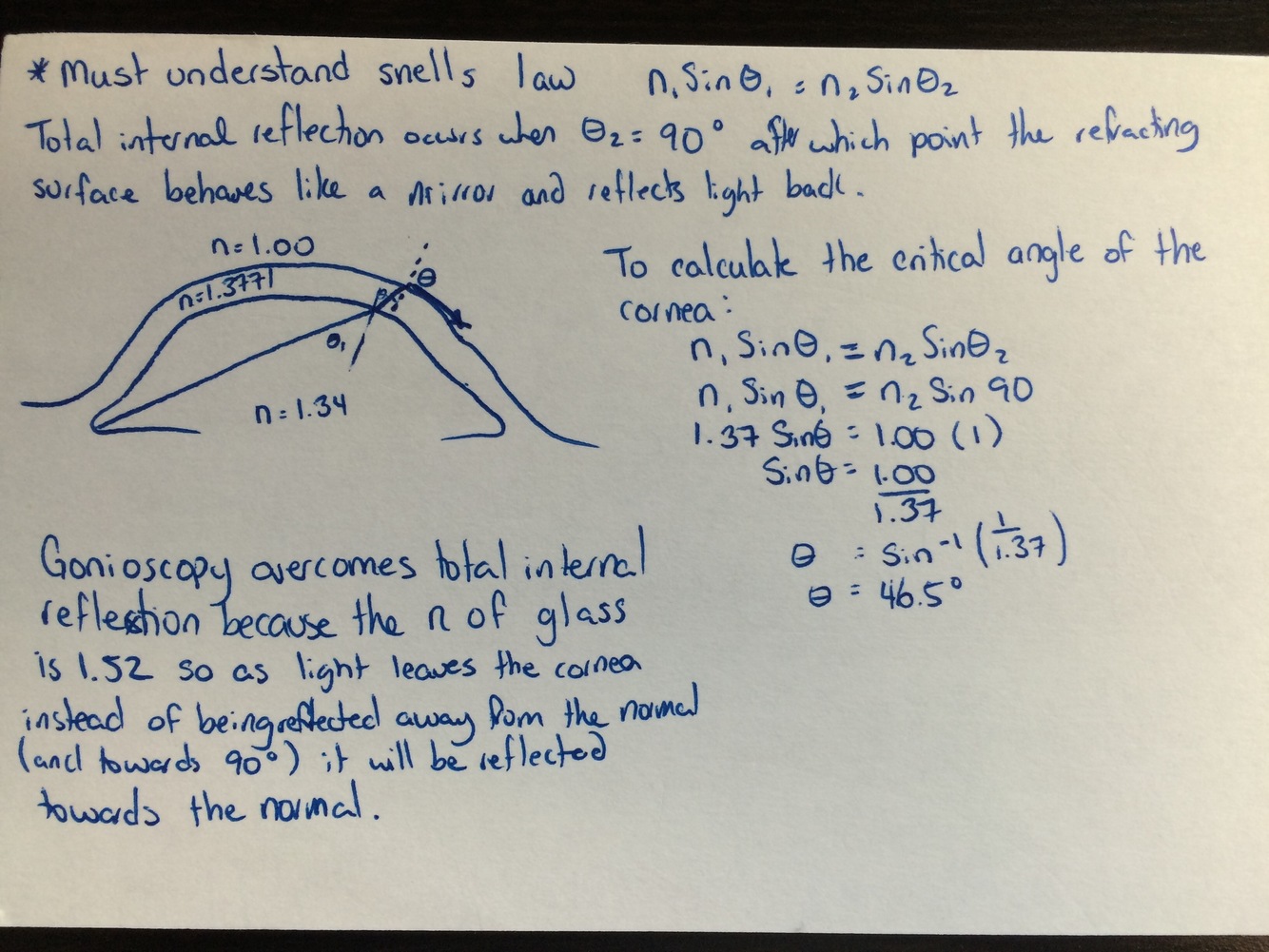
Define and describe how total internal reflection is overcome by gonioscopy
Accomodative Amplitude
Key numbers to remember: at age 40 you have 6D and at age 48 you have 3D.
Before age 40 you loose 1D every 4 years. Between age 40 and 48 you loose 1.5D every four years and then after 48 you loose .5 a diopter per year.
What Add does someone with a certain visual acuity (ex: 20/60) of a certain age(ex. 56) need to read newsprint (J5)?
This question requires you to know what kestenbaums rule is. the required add is the inverse of the acuity (so 20/60 would be 60/20=+3D additional needed.
And then you use their age to determine what accomodative amlitude they already have.
A 52 year old had 3D at age 48 and has lost another .5 diopters every 4 years since then. So they have 2 dipoters left. But its only comfortable to use 1/2 your total available accomodation so they have 1D available.
+3D minus the one they can use = a +2 Add to read newsprint.
Prism Diopter
The amount in cm that an image will be displaced toward the base at 1m.
ex: 10D prism will displace an image 10cm at 1m.
Prentice’s Rule
power of the lens x distance from optical center = prism induced
Define far point
The point in an unaccomodated eye at which rays that have entered parallell have come to a focus.
describe the attached image
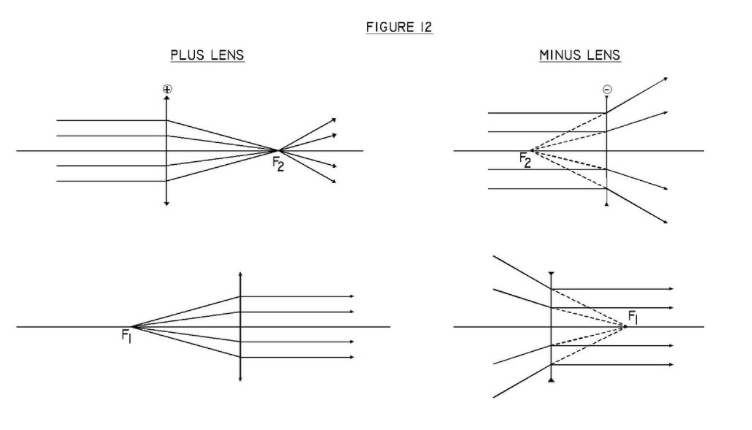
The primary focal point (F1) of a lens is also called the Object-Space Focus.
For a plus lens, this is the point from which light must originate to emerge parallel from the lens. Thus, the image is at infinity.
For a minus lens, this is the point towards which the incident light must be directed in order for the image rays to emerge parallel.
The primary focal length, (f1), is the distance from the optical surface to the primary focal point (F1). Secondary focal point (F2) of a lens is also called the Image-Space Focus.
For a plus lens, this is the point where parallel rays from a distant point object are rejoined to form an image at that point. When parallel rays enter the optical surface, they will focus at the secondary focal point.
For a minus lens, this is the point from which diverging rays seem to come from, after a parallel bundle of rays are refracted by a negative lens.
The secondary focal length, (f2), is the distance from the optical surface to the secondary focal point (F2).
For a plus (+)/convergent lens, the secondary focal point is to the right of the lens.
For a minus (-)/divergent lens, the secondary focal point is to the left of the lens.
Define Near Point
Image Jump
Image Jump is produced by the sudden introduction of the prismatic power at the top of a bifocal segment. The object the individual sees in the inferior field suddenly jumps upward when the eye turns down to look at it. If the optical center of the segment is at the top of the segment, there is no image jump. Image jump is worse in glasses with a round top bifocal, because the optical center of the bifocal is farther from the distance lens optical center. A flat top bifocal is better because the optical center of the bifocal is close to the distance optical center.
Image Displacement
Image Displacement is the prismatic effect induced by the combination of the bifocal type and the power of the distance lens prescription in the reading position. Image displacement is more bothersome than image jump for most people. Most bifocal corrected presbyopes read through a point about 10 mm below the optical center of their distance lenses. If that position is also at the bifocal segment’s optical center, as in most fused flat top bifocals, the bifocal segment produces no prismatic effect at all. The prismatic effect that is there is induced by the distance lens correction, not the segment. However, if the optical center of the bifocal segment is located below or above the reading position, the bifocal will contribute to image displacement at the reading position. The total prismatic displacement will be the sum of that produced by the bifocal and that induced by the distance lens.
Amplitude of accomodation
Total number of diopters an eye can accomodate
Range of accomodation
How does a fibre optic cable work.
-
OPTICS23
-
Retina265
-
Peds161
-
Cornea111
-
Phakomatoses14
-
Optic Neuropathy4
-
General16
-
Ectasia1
-
Dytrophies7
-
Optic Neuropathies1
-
Neuromuscular Diseases2
-
Evidence to know62
-
Meds2
-
Glaucoma149
-
Neuro-Ophthalmology80
-
Plastics/Orbit99
-
Genetics3
-
Syndromes6
-
Lens11
-
Optics48
-
Surgery Specifics1
-
Cornea Pics10
