Explain about Congenital Abnormalities of the Stomach
- Diaphragmatic hernia: If there is incomplete fusion of the primitive diaphragm with a ring of muscle that develops from the body wall, the contents of the abdomen may push up into the pleural cavity forming a diaphragmatic hernia, pushing the heart forwards and compressing the lungs. The incidence is about 1 in 2000 births and treatment is surgical.
- Hypertrophic pyloric stenosis: pyloric stenosis occurs in about 1 in 150 males and 1 in 750 female infants. A genetic factor is involved. Stenosis is caused by hypertrophy of the circular muscles of the pylorus, obstructing the pyloric canal and the flow of contents from the stomach into the duodenum. Stenosis may also be acquired in adult life, usually caused by scarring from peptic ulceration or because of malignancy obstructing the outflow. Diagnosed by barium meal and gastroscopy
Describe gastritis
[*] Gastritis (inflammation of the stomach) may be acute or chronic
- Acute gastritis involves an acute inflammatory reaction at the superficial mucosa with the infiltration of neutrophils. Acute gastritis is almost always caused by drugs (especially NSAIDs such as aspirin) or by alcohol (the most common cause) cuasing chemical exfoliation of the surface epithelial cells and decreasing the secretion of protective mucus.
- The causative drugs or chemicals often inhibit prostaglandins which protect the gastric mucosa by stimulating mucus and HCO3- production and inhibiting acid secretion.
- H. pylori has been implicated in both acute and chronic gastritis.
- NSAIDs such as aspirin inhibit the enzyme cyclooxygenase (COX) which is necessary for prostaglandin production. Concurrent therapy with a proton-pump inhibitor can prevent gastritis and ulcer formation
- Acute erosive gastritis is typified by a partial loss of gastric mucosa. It is caused by shock, severe burns and toxic substances and alcohol.
- Symptoms: discomfort (dyspepsia), epigastric pain and vomiting
Chronic gastritis: chronic inflammatory changes in the mucosa causing atrophy and epithelial metaplasia. Can be autoimmune, bacterial or due to reflux.
- Vitamin B12 is needed for the synthesis of DNA. Normally the nucleus is extruded from red blood cells before they are released into the peripheral blood from the bone marrow. In Vitamin B12 deficiency however maturation of the nucleus is delayed relative to the cytoplasm and macrocytic or megaloblastic blood cells with nuclei are seen in the peripheral blood.
Describe Peptic Ulcer Disease
[*] ulcers arise when damaging factors, particularly gastric secretions, overwhelm the natural protection of the mucosal lining of the GI tract. Acute peptic ulcers are usually caused by the same factors as acute erosive gastritis. Chronic peptic ulcers occur in the upper GI tract where gastric acid and pepsin are present as chronic ulcers are caused by hyperacidity, H. pylori, reflux of duodenal contents, NSAIDS and smoking. Genetic factors also play a role. Males are 3x more likely to develop chronic ulcers than females. There is an increase in incidence of peptic ulcer above the age of 45 years. Both duodenal and gastric ulcers are common in the elderly
- Duodenal ulcers are two to three times more common than gastric ulcers occurring in about 15% of the population. Approximately 90% of DU are associated with H. pylori. Classically the epigastric pain is said to be relieved by food or antacids, and exacerbated by hunger
- 70% of gastric ulcers are associated with H. Pylori with the rest mainly associated with NSAID treatment.
Describe delayed gastric emptying
[*] Delayed gastric emptying: can be delayed by mechanical or non-mechanical obstructions
- Mechanical obstructions: tumours; duodenal, gastric or pyloric stenosis and bezoars (a mass of swallowed foreign material which has collected and is obstructing emptying)
- Non-mechanical delayed gastric emptying is known as gastroparesis. This is an uncommon complication of diabetes (associated with peripheral neuropathy) but can also occur due to gastric arrhythmias, myotonic dystrophy, collagen-vascular diseases, neuropathies and after vagotomy.
Describe benign neoplasms
- Gastrointestinal stromal tumour (GIST, formerly leiomyoma) arising from smooth muscle which may bleed from ulceration. These are the most common benign gastric tumours
- Adenomas (benign tumours of glandular origin) make up 5-10% of polypoid lesions in the stomach and may contain proliferative dysplastic epithelium with the potential for malignant transformation. Much more common in the colon, but if present in the stomach, are usually in the antrum. More common in males and the incidence increases with age
- Fibromas and neurofibromas which are connective tissue tumours
- Hyperplastic polyps (regenerative polyps) are elongated gastric pits separated by fibrous tissue, usually found in association with H. pylori infection in the antrum
Describe malignant neoplasms
- [*] ~15/100000 people in the UK are affected with gastric carcinoma each year and the incidence increases with age, affecting men more than women. It is the fifth biggest cause of death due to malignancy. The incidence is falling in both Europe and the USA although it remains high in the Far East for which dietary factors have been implicated.
- Adenocarcinoma is the most common gastric neoplasm and accounts for 90% of all malignant neoplasms in the stomach. Malignant lymphomas account for 5% of gastric malignant neoplasms and other malignancies such as carcinoid and malignant spindle cell tumours occur rarely.
- A number of conditions are premalignant such as atrophic gastritis, some chronic gastric ulcers, pernicious anaemia and post-gastrectomy (carcinomas often develop 15-20 years after surgery)
- Genetic factors may also be involved e.g. incidence is slightly higher in blood group A
- H. pylori infections cause chronic gastritis which occasionally becomes atrophic gastritis, leading to metaplasia, dysplasia and ultimately carcinoma
- Dietary factors may act to initiate or promote carcinogenesis. A diet high in salt increases in the risk. Also dietary nitrates are converted to carcinogenic nitroasmines by bacteria. Therefore diets high in nitrates predispose to carcinoma (the incidence is high in Japan). Diets high in fruit and vegetables can help protect against cancer because of the antioxidants they contain
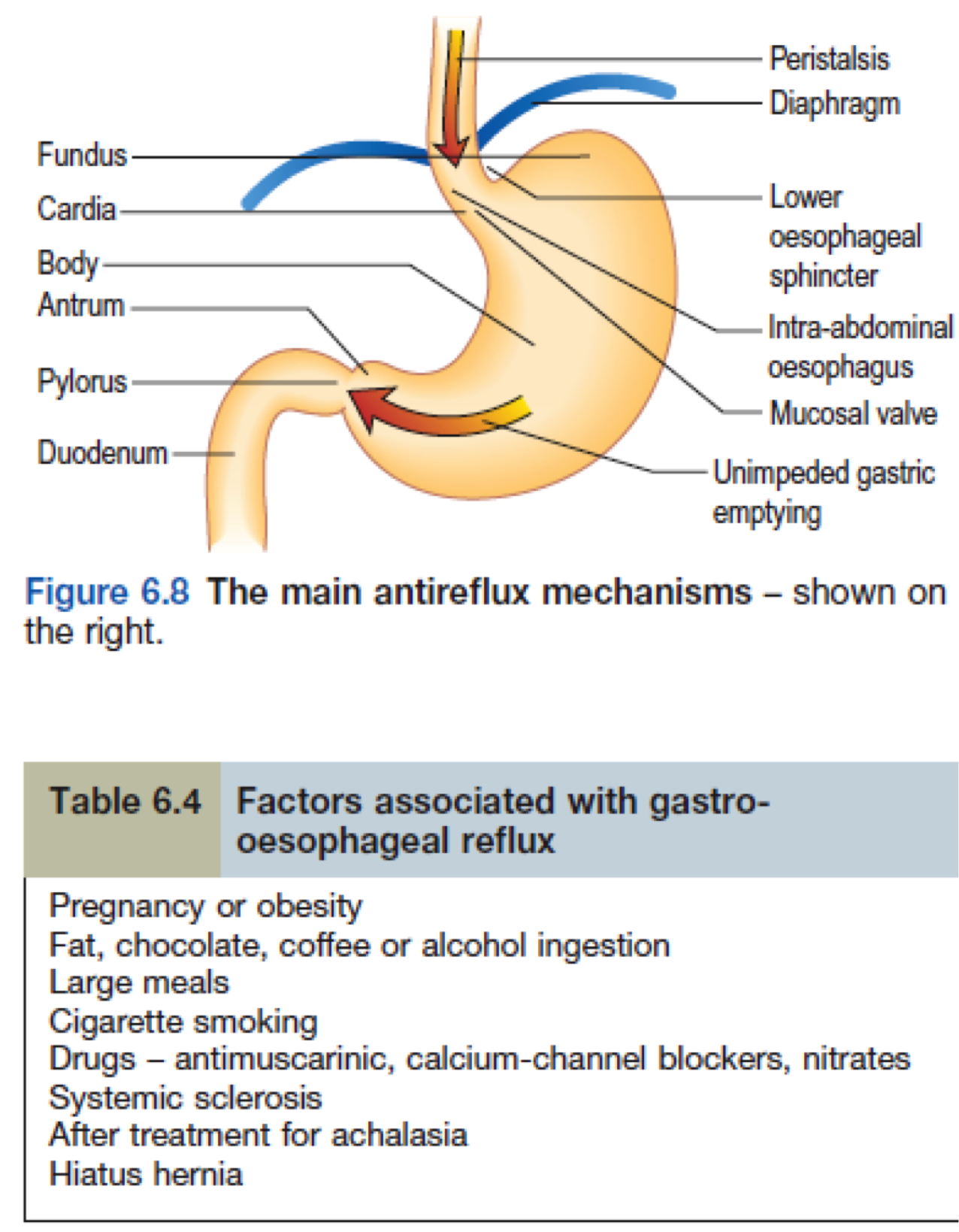
What are the anti-reflux mechanisms?
- Lower oesophageal sphincter which is usually closed and transiently relaxes as part of physiology of swallowing to allow bolus to move into stomach
- Oesophagus enters stomach in abdominal cavity at an oblique angle (valve-like effect)
- Pressure in abdominal cavity is higher than that of thoracic
- Right crus of diaphragm acts as sling around the lower oesophagus
- Plug like action of the mucosal folds
- Some acid reflux is normal and this is normally dealt with by secondary peristaltic waves, gravity and salivary bicarbonate
What are the clinical features and investigations of GORD?
Clinical features occur when antireflux mechanisms fail and there is prolonged contact of gastric juices with lower oesophageal mucosa
[*] Clinical features: dyspepsia (heartburn/indigestion) – worse on lying down, bending over and drinking hot drinks
[*] Investigations and diagnosis: usually clinically diagnosis made without investigation on symptoms alone – no need to investigate unless alarming symptoms such as dysphagia or hiatus hernia is suspected (which would be investigated by endoscopy)
Describe the management and complications of GORD
- Lifestyle (lose weight, stop smoking, reduce alcohol consumption, reduce consumption of food groups known to aggravate (e.g. chocolate, fatty foods)
- Medication (simple antacids e.g. calcium carbonate (neutralises acid); raft antacids (alginates) e.g. Gaviscon liquid, taken after eating which creates protective raft that sits on top of stomach contents to prevent reflux
- Proton Pump inhibits e.g. omeprazole which causes a reduction in acid secretion by parietal cells
- H2 antagonists e.g. ranitidine which blocks H2 receptors and reduces acid secretion
[*] Complications: continual contact of gastric juices with oesophageal mucosa can lead to metaplastic change => Barrett’s Oesophagus
What are peptic ulcers? Describe their cause and epidemiology
[*] Peptic ulcers break through superficial epithelial cells, penetrating down into Muscularis mucosa of either stomach or duodenum. Most duodenal ulcers are found in duodenal cap and gastric ulcers are most commonly seen in lesser curvature of stomach
[*] Causes:
Leading cause in the developed world is use of NSAIDs which inhibit production of prostaglandins, preventing production of protective unstirred layer. 50% of patients taking long term NSAIDs have mucosal damage and 30% when endoscoped have peptic ulceration but only 5% will be symptomatic and only 1-2% will have complications such as GI bleed
[*] Epidemiology duodenal ulcers found in ~10% adult population and are 2-3 times more common than GUs. Prevalance is falling for young people (especially men) and increasing in older people (especially older women). In developed countries increased prevalence of NSAID associated DUs and decreasing prevalence of H pylori associated ulceration
Describe the clinical features, investigations and management of Peptic Ulcers
[*] Clinical features:
- Recurrent, burning epigastric pain (pain is often worse at night and when hungry with duodenal ulcers and relieved when eating). Pain may subside with antacids.
- Persistent severe pain suggest penetration of ulcer into other organs
- Back pain suggest penetrating posterior ulcer
- Can also get nausea, vomiting (though less common)
- With GUs, can get weight loss and anorexia
- May be asymptomatic and present for first time with hematemesis (vomiting of blood) when ulcer has perforated blood vessels
[*] Inbestigations:
- Investigate H Pylori infection
- In older patients (over 55y/o) or with other alarming symptoms => endoscopy to exclude cancer
[*] Management:
- If due to H pylori infection => triple therapy
- Proton Pump inhibitor: omeprazole
- Antibiotics: Clarithromyocin and Amoxicillin/Metronidazole
- HH2 antagonist – Cimetidine
- If taking NSAIDS, stop or review – use alternatives (NSAIDs with lower risk of causing PUD or using prophylactic PPI as well as NSAID)
What are complications of Peptic Ulcer Disease?
- Haemorrhage of blood vessels which ulcer has eroded => presents with hematemesis and melena (black, tarry stools)
- Perforation of the ulcer – more common in DUs than GUs – usually perforate into peritoneal cavity
- Gastric outlet obstruction => can be pre-pyloric, pyloric or duodenal. Occurs either because of active ulcer with oedema or due to healing of an ulcer with associated fibrosis (scarring). Gastric outlet obstruction normally presents as vomiting without pain.
Describe the pathophysiological features of Helicobacter pylori?
H pylori is a gram negative, aerobic helical, urease producing bacterium that resides in the stomach of infected individuals
- Motile (burrow into mucous gel)
- Microaerophilic
- Adheres to gastric mucosa
- Produces cytotoxins
- Transmission (cohort effect – elderly people got it when they were children and have kept it all of their life, children these days have far less exposure so they are less likely to get it – food hygiene practice, household cleanliness etc have changed). It is thought to be ingested by children. Colonization can occur for years and years
- Associated with gastritis – mounts an immune response via cytokines
- Production of urease produces ammonia (by breaking down urea into carbon dioxide and ammonium ions), which neutralises acidic environment, allowing bacterium to survive.
- It colonises gastric epithelium – in mucous layer or just beneath. Damage to epithelia occurs through enzymes released and through induction of apoptosis. Damage also occurs due to the inflammatory response to the infection (inflammatory cells and mediators). Because of the acidity, no other bacteria colonizes the stomach.
TNF, IL1 IF stimulate gastrin secretion
TNF decreases antral D cells
Vitamin C inhibits gastric cancer cell growth
Describe the diagnosis and treatment of Helicobacter pylori
[*] Diagnosis:
- IgG detected in serum (relatively good sensitivity and specificity)
- C-urea breath test (C-urea ingested – if H pylori present, the urease produced will break C-Urea to NH3 and CO2. CO2 will be exhaled on breath and detected).
- Can also take gastric sample by endoscopy and detect by histology and culture
[*] Treatment:
- Proton pump inhibitor – omeprazole
- Two antibiotics: Clarithromyocin, Amoxicillin
- H2 antagonist (if severe)
- This standard eradication therapy, depending on local resistance, is successful at eradicating infection in 90% of patients.
- 7-14 day treat – 14 days more effective but side-effects of treatment may put patients off finishing two week course.
Describe H pylori causing gastric disease
- Gastritis: usual effect of infection, which is usually asymptomatic. Chronic gastritis causes hypergastrinaemia due to gastrin release astral G cells => this increased acid production is usually asymptomatic but can lead to duodenal ulceration (which will eventually produce symptoms)
- Peptic ulcer disease
- Duodenal ulcers: prevalence of DUs due to H pylori is falling due to decreased prevalence of H pylori infection. If ulcers due to H pylori infection, eradication of infection relieves symptoms and decreases chances of recurrence. The precise mechanism of ulceration is unclear (only occurs in 15% of infected people) but factors implicated though are genetic predispositions, bacterial virulence, increased gastrin secretion and smoking
- Gastric ulcers: associated with gastritis affecting the body of the stomach as well as the antrum which can cause parietal cell loss and reduction in acid production. Ulceration is thought to occur due to reduction in gastric mucosal resistance due to cytokine production as a result of infection.
- Gastric cancer
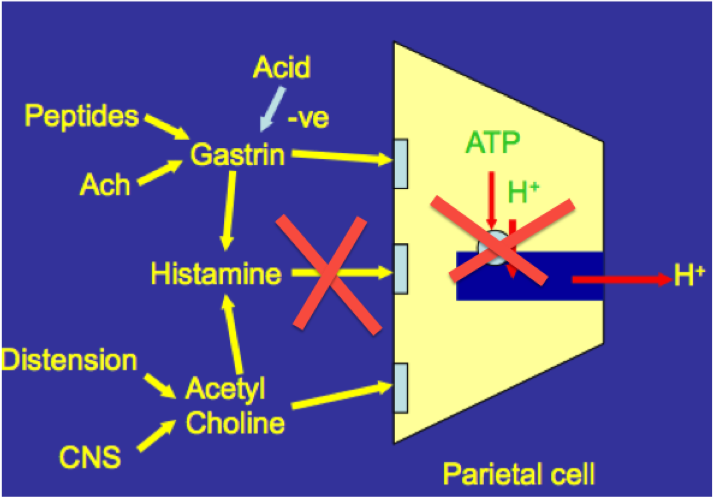
Outline the ways in which gastric acid secretion may be reduced by drugs
[*] Acid secretion may reduced by inhibiton of Histamine at H2 receptors e.g. Cimetidine which removes the amplification of Gastrin/ACh signal
[*] Protein pump inhibitors e.g. omeprazole prevent H+ ions being pump into parietal cell canaliculi
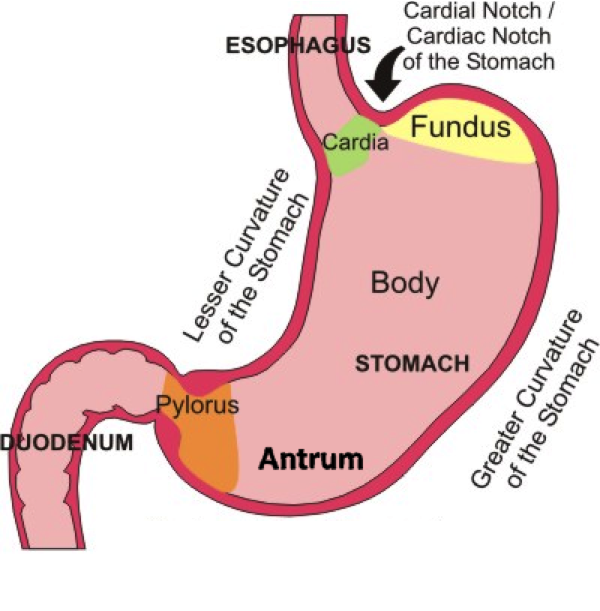
Describe the gross structure and parts of the stomach
[*] The stomach is the expanded part of the GI tract between the oesophagus and duodenum, between the levels of T7 and L3 vertebrae
[*] J-shaped curve
[*] It is specialized for the accumulation of ingested food – can hold 2/3 litres of food.
[*] The shape and position of the stomach varies, depending upon body shape, degree of distension and posture. In supine position, the stomach lies in the right and left upper quadrants or epigastric, umbilical, left hypochondrium and flank regions.
[*] The cardia surrounds the superior opening of the stomach
[*] The fundus is the rounded portion superior to and left of the cardia
[*] The body is the large central portion inferior to the fundus
[*] The pylorus connects the stomach to the duodenum.
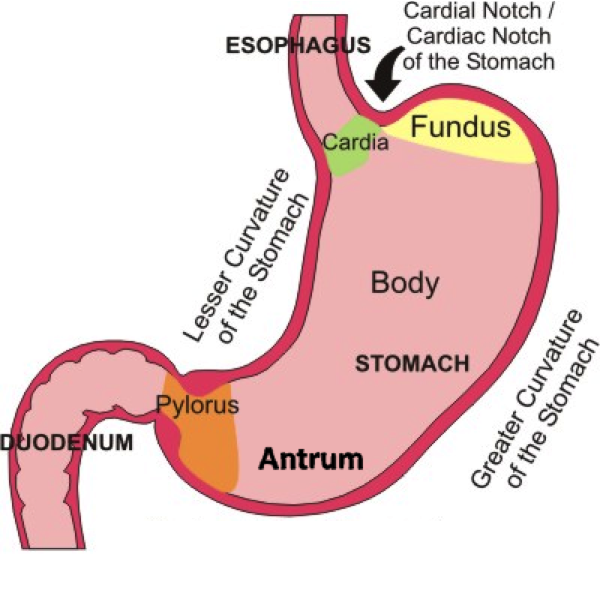
Describe the curvatures of the stomach
[*] The greater curvature forms the long convex lateral border of the stomach. It arises from the cardiac orifice, arches backwards and passes inferiorly to the left. It curves to the right as it continues medially to reach the pyloric antrum. The short gastric arteries and the right and left gastro-omental (gastroepiploic) supply branches to the greater curvature.
[*] The lesser curvature forms the shorter concave medial surface of the stomach. The most inferior part of the lesser curvature, the angular incisures indicates the junction of the body and pyloric region. The lesser curvature gives attachment to the hepatogastric ligament and is supplied b the left gastric artery and the right gastric branch of the hepatic artery.
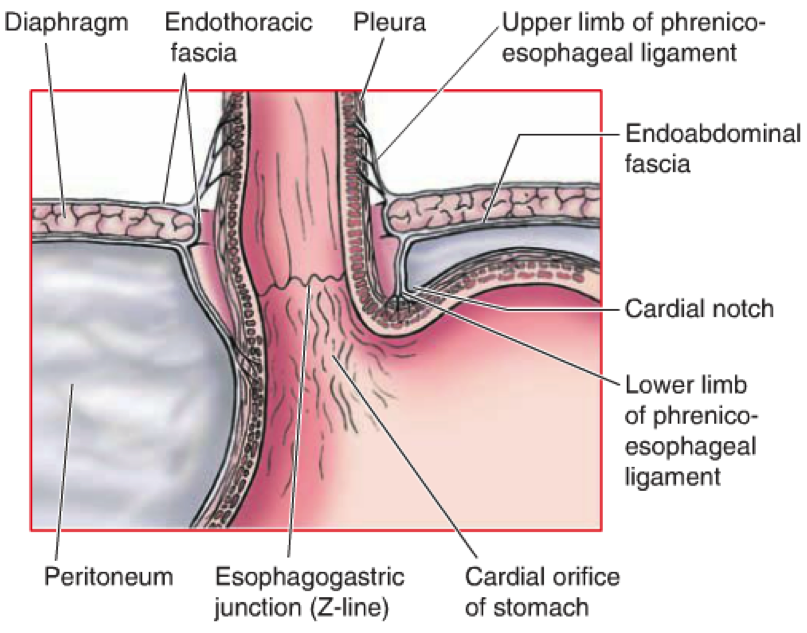
Describe the inferior oesophageal sphincter
[*] Inferior Oesophageal Sphincter: the oesophagogastric junction lies to the left of the T11 vertebra on the horizontal plane that passes through the tip of the xiphoid process. The line where the mucosa abruptly changes from oesophageal to gastric is known as the Z-line.
- Immediately superior to the Z-line, the diaphragmatic musculature forming the oesophageal hiatus functions as a physiological sphincter that contracts and relaxes. This, coupled with the cardiac notch prevents reflux of stomach contents
- At the oesophageal hiatus, the right crus exerts pressure on the oesophageal wall
- In the normal (non-eating state), the lumen of the oesophagus is collapsed. The oesophagus enters the stomach at an angle – when the stomach is full, this closes off entry to the sphincter
- However reflux of gastric contents into the oesophagus is common. If it is frequent and/or clearance of reflux material is deficient, “heartburn” and/or inflammation with ulceration may result. Chronic reflux may result in metaplastic changes in the mucosa (Barrett’s oesophagus)
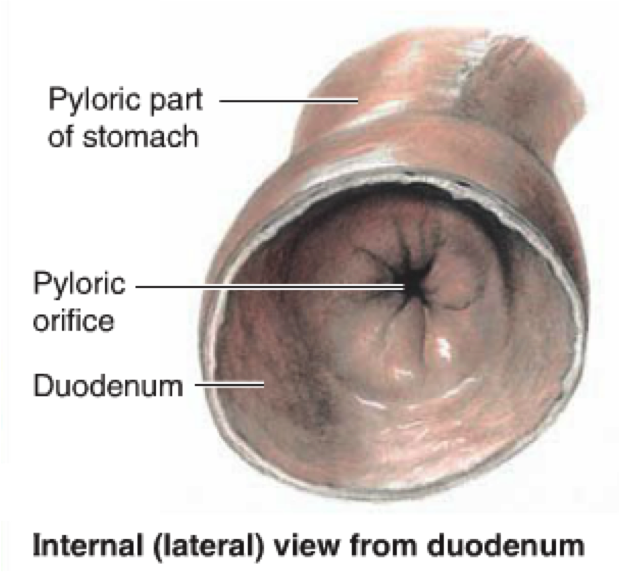
Describe the pyloric sphincter
[*] Pyloric sphincter: at the pyloric end of the stomach, the circular muscle coat is thickened to produce the pyloric sphincter. This controls the discharge of the stomach contents through the pyloric orifice into the duodenum
- In contrast to the inferior oesophageal sphincter, this is an anatomical sphincter. It contains smooth muscle which thickens to control the discharge of stomach contents through the orifice.
- Emptying the stomach occurs intermittently when intragastric pressure overcomes the resistance of the pylorus. The pylorus is normally tonically contracted so that the orifice is small and food can stay in the stomach for a suitable period. Gastric peristalsis pushes the chyme through the pyloric canal into the duodenum for further digestion.
Describe the macro and microscopic structure of the gastric mucosa
[*] When empty the gastric mucosa is thrown into longitudinal folds called rugae, and a gastric canal forms temporarily between the gastric folds along the lesser curvature to allow saliva and other fluids (and small amounts of chewed food) to pass along to the pylorus.
[*] The Gastric mucosa has 3 histologically distinct zones:
- Cardia: neck cells – mucus
- Fundus and Body: neck cells – mucus; parietal – acid; chief – pepsinogen
- Pyloric: neck cells – mucus; G-cells - Gastrin
Peptic ulcers commonly occur in the antrum and along the lesser curvature of the stomach. Perforation of ulcers leads to the spillage of gastric contents into the peritoneal cavity, which may affect abdominal structures such as the pancreas and associated blood vessels lying in close proximity to the stomach.
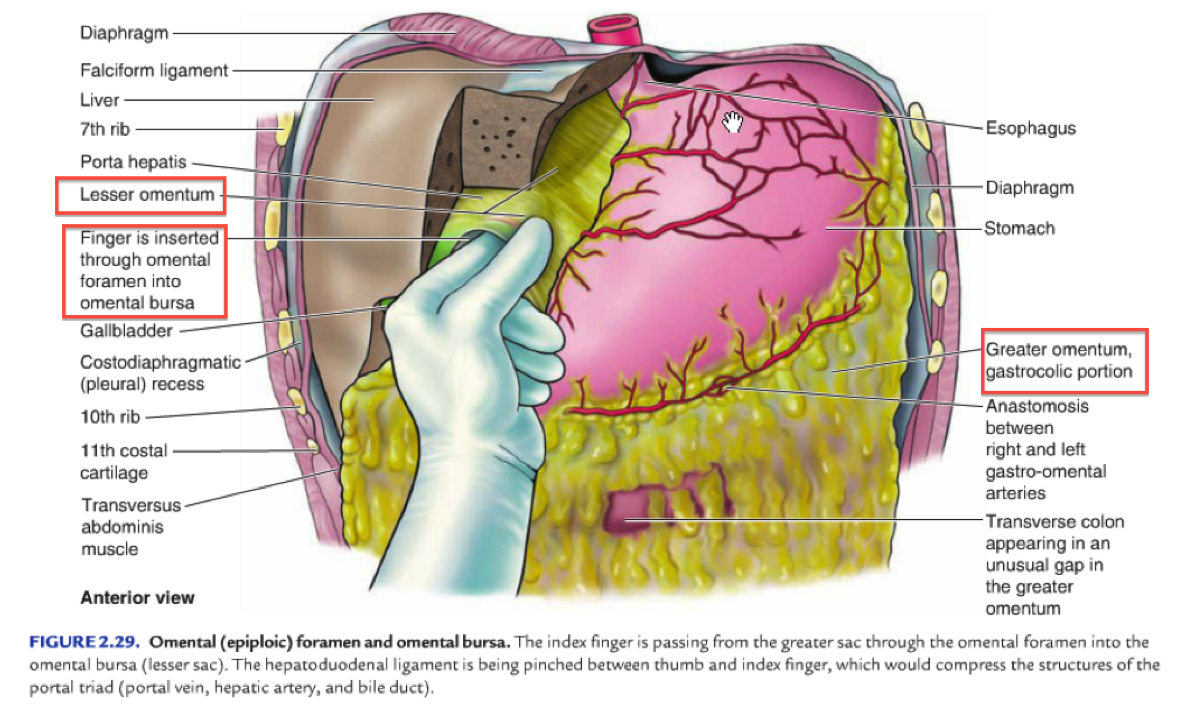
Describe the greater and lesser omenta
- Greater Omentum: a prominent, four-layered peritoneal fold that hangs down like an apron from the Greater Curvature. After descending it folds back and attaches to the anterior surface of the transverse colon and its mesentery. Then it folds back upon itself before reaching the posterior abdominal wall. It features many lymph nodes which contain macrophages to combat infections of the GI tract.
- Lesser Omentum: a much smaller double-layered peritoneal fold which connects the lesser curvature and the proximal part of the duodenum to the liver. It also connects the stomach to the portal triad (distinctive arrangement in the liver: proper hepatic artery, hepatic portal vein, common bile duct + lymphatic vessels and branch of vagus nerve)
- Together the greater and less omenta divide the abdominal sac into two: the greater and lesser sac. The stomach lies immediately anterior to the lesser sac.
Describe the celiac trunk
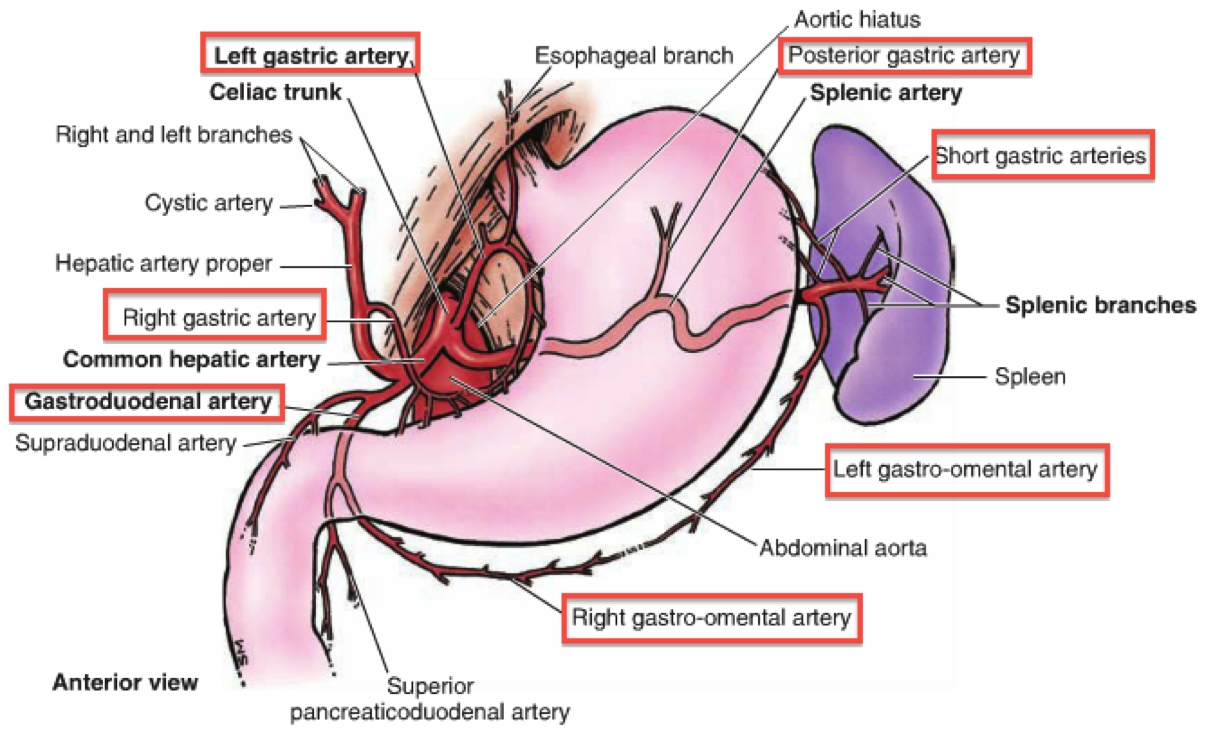
- The coeliac trunk originates from the abdominal aorta, giving rise to the left gastric, splenic and common hepatic arteries
- Branches from the aorta at T12 vertebra
- Left gastric artery branches: oesophageal branch, stomach branch
- Common hepatic artery branches: proper hepatic artery, right gastric artery, gastroduodenal artery
- Splenic artery: dorsal pancreatic artery, short gastric arteries, left gastro-epiploic artery, greater pancreatic arter
- Coeliac trunk may also give rise to the inferior phrenic arteries
- Supplies the forgut: liver, stomach, abdominal oesophagus, spleen and superior half of both the duodenum and the pancreas
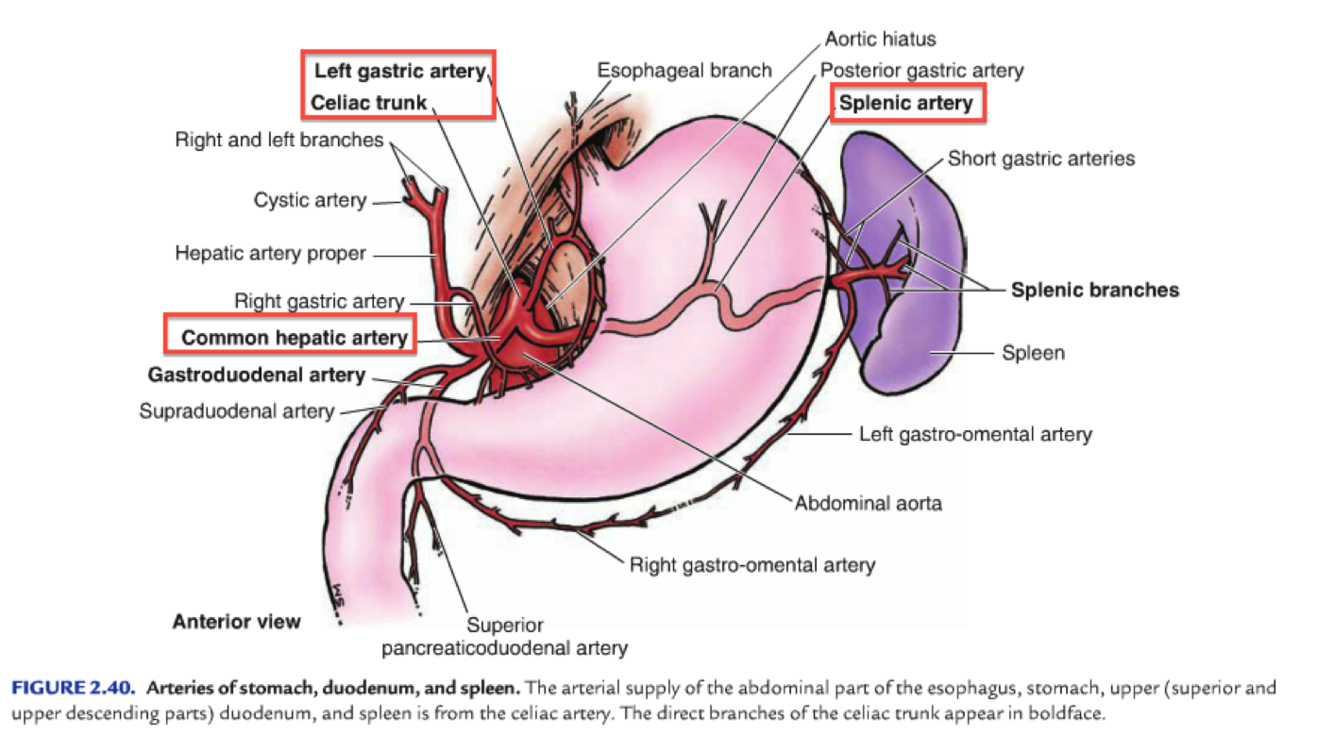
Describe the arterial supply of the stomach
The rich arterial blood supply of the stomach arises from the coeliac trunk and its branches
Lesser Curvature:
- Coeliac Trunk => Left Gastric
- Coeliac Trunk => Common Hepatic => Right Gastric
Greater Curvature:
- Coeliac Trunk => Splenic => Left Gastro-epiploic
- Coeliac Trunk => Common Hepatic => Gastroduodenal => Right Gastro-epiploic
Fundus and Body:
- Coeliac Trunk => Splenic => Posterior Gastric / Small Gastric
- Anastomoses from along the lesser curvature by the right and left gastric arteries and along the greater curvature by the right and left gastro-epiploic arteries.