What are the neck fascia?
A. Superficial cervical fascia
- lies between dermis and investing layer of deep cervical fascia
- contains the plastysma, and cutaneous vessels, nerves, lymphatics, fats
B. Deep cervical fascia
- *1) Investing layer of deep cervical fascia**
- contains SCM and trapezius
- arises from skull superiorly, attach to scapular spine, acromion, and clavicles inferiorly
- *2) Pretracheal fascia**
- anterior neck only
- extends inferiorly from hyoid bone into the thorax, merges with fibrous pericardium
- contains thyroid, trachea, esophagus
- *3) Prevertebral fascia**
- from base of skull to T3 vertebra
- contains vertebral column and associated muscles
- extends laterally as axillary sheath
4) Carotid sheath
How might deep fascia influence the spread of infection from the neck?
The neck fascia determines the direction in which a neck infection may spread:
- the investing layer of deep cervical fascia prevents the spread of abscesses
- if investing layer is breached, an infection between the investing and pre-tracheal layer can spread inferiorly to the thoracic cavity anterior to fibrous pericardium
- if abscess is located posterior to the pre-vertebral fascia, then it can extend laterally
What are the main neck muscles
i) innervation
ii) attachment
iii) function
- *1) Platysma**
i) innervated by CN VII (facial nerve)
ii) attach from mandible to pectoral muscle
iii) function: draws down corners of mouth - *2) Sternocleidomastoid (SCM)**
i) innervated by CN XI (accessory nerve)
ii) attach from mastoid to manubrium and clavicular head
iii) function: rotates head - *3) Trapezius**
i) innervated by CN XI (accessory nerve)
ii) Originates from occiput and spinous processes, cervical and thoracic vertebrae; inserts to scapular and clavicle
iii) function: elevates scapula
Where is the root of the neck?
- what is the boundaries
- what are the contents
Root of the neck refers to the junction between the thorax and neck, where structures pass from thorax to head:
- *Boundary:**
- anterior: manubrium
- posterior: body of T1
- lateral: 1st rib and costal cartilage
- *Contents:**
- Arteries: Brachiocephalic trunk (R), left CCA, left subclavian artery
- Veins: anterior jugular vein and IJV forms brachiocephalic vein, and EJV / subclavian vein
- Nerves: vagus nerve, RLN, phrenic nerve, sympathetic trunks, cervical sympathetic ganglia
What are the anatomical zones of the neck?
What is its clinical relevance?
Zone I
- from sternoclavicular notch to cricoid carilage
- vulnerable structures: cervcial pleura, lung apex, thyroid, trachea, esophagus, jugular vein, cervical vertebrae
Zone II
- from cricoid cartilage to angle of mandible
- vulnerable structures: larynx, pharynx, carotids, jugular vein, cervical vertebrae
Zone III
- from angle of mandible to base of skull
- vulnerable structures: oropharynx, oral cavity, nasal cavity
==================
It is used to describe penetrating trauma to neck:
-> Zone II is the most exposed zone, and is consequently the most likely to be injured; but best prognosis
-> Zone I and III has greatest morbidity and mortality, because:
i) may obstruct airway
ii) injured structures are difficult to visualise
iii) harder to control vascular damage by direct pressure in comparison to Zone II
Levels of neck LN
- *1a: Submental
1b: Submandibular** - *2: Upper jugular**
- from base of skull, to inferior border of the hyoid bone
- *3: Middle jugular**
- from inferior border of the hyoid bone, to inferior border of cricoid cartilage
- *4: Lower jugular**
- from inferior border of cricoid cartilage, to clavicles
- *5a: Posterior triangle
5b: Supraclavicular fossa** - *6: Anterior compartment**
- Pretracheal, paratracheal, precricoid (Delphian) and perithyroid nodes
7: Upper mediastinal
Drainage of neck lymph nodes
Level I
- Anterior nasal cavity
- Oral cavity
- FOM, tongue
Level II
- Nasal cavity, para-nasal sinus, nasopharynx
- Oral cavity, orophaynx
- Hypopharynx, supraglottic larynx
- Parotid and submanidbular glands
Level III
- oropharynx, hypopharynx, larynx
Level IV
- hypopharynx, larynx
- cervical esophagus
- thyroid
Level V
- oropharynx, nasopharynx
- posterior neck and scalp
Level VI
- thyroid
Anterior & posterior neck triangle borders
- *Anterior triangle:**
- Inferior aspect of mandible
- anterior border of SCM
- anterior midline
- *Posterior triangle:**
- Posterior border of SCM
- Anterior border of trapezius
- Clavicle
Content in the posterior neck triangle
“SEreBII”:
1) Subclavian artery
2) External jugular vein
3) Brachial plexus (trunk)
4) CN XI

Borders of Sub-triangles in Anterior neck triangle
- *1) Submental**
- inferior border of mandible
- anterior belly of digastric
- hyoid
- *2) Submandibular**
- inferior aspect of mandible
- anterior & posterior belly of digastric
- *3) Carotid**
- posterior belly of digastric
- superior belly of omohyoid
- anterior border of SCM
- *4) Muscular**
- superior belly of omohyoid
- anterior border of SCM
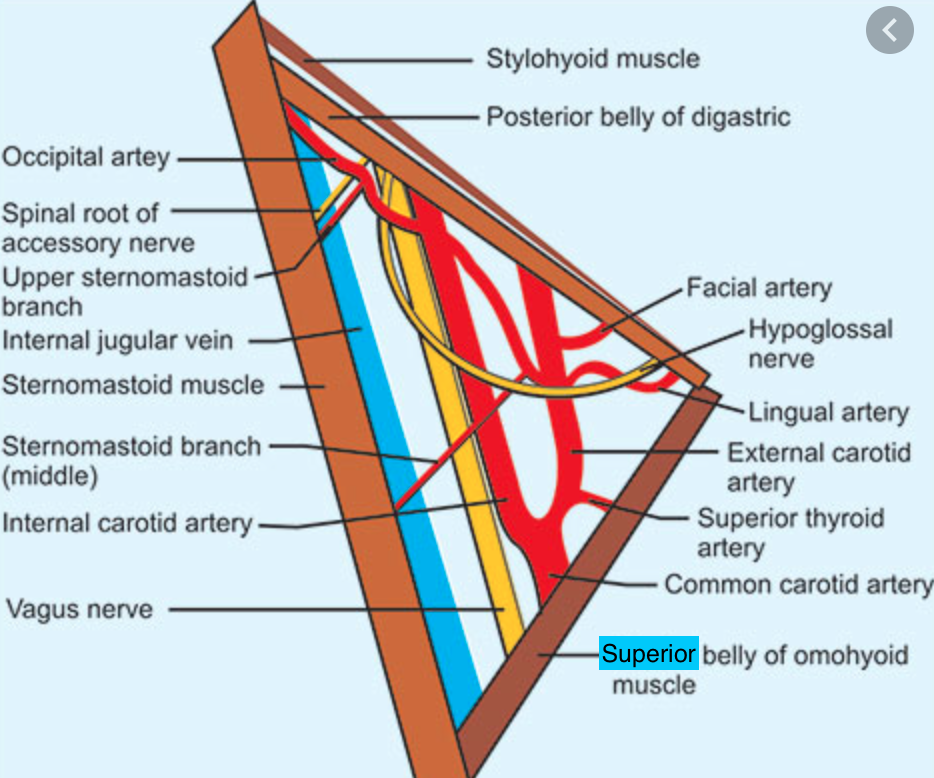
Content in the carotid triangle
- *1) Carotid sheath**
i) common carotid artery (medially)
ii) IJV (laterally)
iii) vagus nerve CN X (posteriorly at the middle) - *2) Ansa cervicalis**
- lies within the anterior wall of the sheath over the jugular vein
3) Hypoglossal nerve CN XII
Define Neck dissection terminologies
- *1) Radical Neck Dissection:**
- ipsilateral level 1-5
- SCM
- spinal accessory nerve
- internal jugular vein
- *2) Modified radical neck dissection**
- ipsilateral level 1-5
- preserve 1+ of (SCM, spinal accessory nerve, IJV)
- *3) Functional neck dissection**
- ipsilateral level 1-5
- preserve all of SCM, spinal accessory nerve, IJV
- *4) Selective Neck Dissection**
- preservation of 1 or more of level 1-5 LN
- Supraomohyoid SND (Level 1-3)
- Lateral SND (Level 2-4)
- Postero-lateral SND (Level 2-5)
- *5) Extended Neck Dissection**
- Radical neck dissection
- and 1+ additional LN groups or nonlymphatic structures
- *6) Central compartment dissection**
- dissection of level 6 only (usu for thyroid)
Selective neck dissection in HnN cancers
Oral cavity cancer:
- Selective 1-3 (aka supraomohyoid SND)
+ level 4 in tongue cancer because of skip lesion
- *Orophaynx, hypopharynx, larynx:**
- Selective 2-4 (aka lateral SND)
- *H&N skin cancer:**
- Selective 2-5 (aka posterolateral SND)
Drainage of pharyngeal cancer to cervical LN
- *1) Nasopharynx (NPC):**
- Level 2-5
- *2) Oropharynx:**
- Level 1-3
- *3) Laryngo-pharynx:**
- Level 2-6
General Mx approach to HnN cancers
- *1) Resection**
- preserve important organ functions
- oncologically clear margins
2) Reconstruction
3) ± Neck dissection
4) Rehabilitation
Margins of resection for skin tumours on head
Squamous cell carcinoma: 1-2cm
Basal cell carcinoma: 3-5mm
Melanoma: 5-50mm
Dermatofibrosarcoma protuberans: 3-5cm
Common histology of H&N cancer
90% is Squamous Cell carcinoma
Common sites of HnN cancers
1) Nasopharynx: fossa of Rosenmuller
- *2) Oral**
- tongue (most common)
- buccal mucosa, lips, floor of mouth, hard palate
- *3) Oropharyx**
- Tonsil (most common)
- tongue base > soft palate
- *4) Hypopharynx**
- Piriform fossa (most common)
- post cricoid > posterior pharyngeal wall
- *5) Larynx**
- glottic > supraglottic > subglottic
Risk factors for Head and Neck cancer (SqCC)
- *Environement factor**
1) Smoking
2) Spirits, alcohol
3) Sharp teeth
4) Betel nut chewing (嚼檳榔 in TW)
5) Previous H&N RT
Patient factor
1) Male Sex (M:F = 4:1)
2) Dental Sepsis
3) Syphilis, HPV
4) GERD
5) Primary H&N tumour (synchronous tumours)
6) Family history
________
think about 6S of oral cancer:
- smoking, spirits, sex, syphilia HPV, sharp teeth, sepsis dental
Ix in head and neck tumours
- *1) Incisional biopsy**
- NOT excisional
- *2) USG, FNAC**
- mass or LN
3) Pan-endoscopy ± biopsy
to look for SYNCHRONOUS tumours
- flexible rhinoscopy
- flexible laryngoscopy
- OGD
- bronchoscopy
- *4) CT, MRI of H&N**
- T, N staging
- look for boney erosion in skull base, orbit
- *5) PET/CT, Bone scan**
- for distant & bone met
Staging of H&N tumours
TNM staging is same except nasal cavity & nasopharynx
T (2-4)
T1: <2cm
T2: 2-4cm
T3: >4cm
T4: adjacent structure
N (3-6) based on size
N1: <3cm
N2: 3-6cm
a: single; b= multiple; c = bilateral
N3: >6cm
M
M1: met
history taking of symptoms Head and Neck cancer (pre-op)
1) Primary Symptoms
2) Symptoms suggestive of synchronous tumours (ask ALL)
Nose
- epistaxis; blood mixed in sputum
- nasal obstruction
- post nasal drip
Ear
- hearing loss
- tinnitis
- otalgia
Mouth
- mass, ulcers, pain
- blood in saliva
- trismus
- loose teeth
Throat
- sore throat
- hoarseness
- dyspnoea
- dysphagia
- haemoptysis
- *3) Metastatic symptoms**
- local: visual, headache, neurological
- lymph: lymph nodes
- distant: lung as SOB, bone pain
Additional aspects affected by H&N cancers
(ask these in history!)
As H&N is the most exposed area of body, will affect morphology & physiology:
- *1) Morphology**
- affects external appearance & aesthetics
- psycho-social complications
- *2) Physiology** (as large number of vital organs in small area):
- vision
- airway
- taste
- swallowing
- speech
Major functions requiring rehabilitation after HnN cancer surgery
- *1) Vision**
- reduced visual acuity from CNII infiltration or RT
- dry eyes (post RT)
- epiphora: lacrimal drainage onbstruction from surgery
- diplopia from muscle impingement
- dystopia from orbital floor invasion
- *2) Airway obstruction**
- temporary oedema
- permanent stricture
- *3) Taste**
- temporary loss of taste (chemo)
- permanent after RT or surgery
- *4) Swallowing**
- immediately dysphagia after glossectomy or pharyngectomy
- delayed dysphagia post RT
- *5) Speech**
- Loss of phonation (post laryngectomy)
- Loss of articulation (glossectomy, nasal, paranasal sinus surgery)






















-
ANATOMY - Lower limbs218
-
Paeds47
-
BREAST114
-
ANATOMY - MALE REPRODUCTIVE SYSTEM179
-
Endocrinology - Diabetes127
-
CARDIOLOGY - ACS and Angina112
-
CARDIOLOGY - Valvular Heart Disease and Bacterial Endocarditis61
-
UROLOGY - Bladder + Prostate52
-
ANATOMY - PELVIS154
-
Neuro - Neurological emergencies72
-
Neuro - stroke, MMA, VST + brain haemorrhages80
-
Neurosurgery183
-
Endocrine Surgery141
-
NEURO - Headache, neuro-oncology and CNS infections91
-
Head & Neck, ENT233
-
MaxFax9
-
ANATOMY - Lower limbs p2232
-
ANATOMY - head205
-
ANATOMY - Neck p1205
-
ANATOMY - Thorax p1199
-
ANATOMY - thorax p2155
-
ANATOMY - Upper limb p1205
-
Miscellaneous28
-
ANATOMY - Head part 299
-
ANATOMY - Upper limb p2205
-
ANATOMY - Abdomen p1209
-
ANATOMY - Abdomen p2215
-
ANATOMY - Abdomen p3127
-
ANATOMY - head part 3190
-
Miscellaneous stuff I get wrong p1200
-
ANATOMY - Neck p2122
-
Vascular from eMRCS1
-
Miscellaneous stuff I get wrong - part 2106
-
ANATOMY - upper limb p392
-
Burns/Grafts/Organ Transplants73
-
Surgeries key facts14
