Action potential graphs comparison between atrium, ventricle and SA node.
Atrium reaches peak quickly and drops with no plateau but a slow drop, ventricle peaks very shortly after followed by a plateau, SA node peaks first with an equal rise and drop.
SA node action potential
The nodal cell action potential is easy to recognize since there is no plateau phase, the depolarization phase is slower than in the atrial or ventricular cell and the resting membrane potential is achieved briefly as the cell continues to depolarize automatically until the next action potential is triggered.
Divisions of the action potential in the ventricular cell
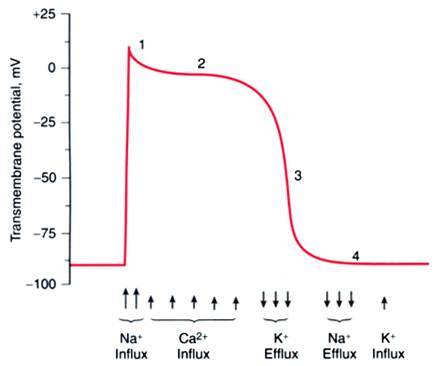
Phase 0 is the rapid depolarization, phase 1 is a transient repolarization, phase 2 is the plateau phase where the contraction happens, phase 3 is the repolarization phase and phase 4 is the resting potential phase.
Membrane potential regarding ion influx in phases of action potential in a fast fiber
Graph of the channels in slow fiber action potential
Phase 0 of the fast fiber action potential
- at -90mv, gates closed but small chemical gradient and large electrical gradient, 2. at -65mv, gate is open and Na+ runs through following electrical and chemical gradient. 3. At 0mv, no electrical gradient but Na follows chemical gradient, 4. at +20mv it continues to follow the chemical gradient but is opposed by the electrical gradient, 5. at +30mv the channel is closed and Na+ can’t enter because the electrical gradient overpowers the chemical gradient.
What are the two sodium channel gates?
m (activation gates) and h (inactivation gates).
Where does transient outward current occur?
Phase 1
Where does the Delayed rectifier current occur?
Phase 1 and 3
Where does the inwardly rectified current (Ikl) occur?
Phase 1 and 4, during repolarization from -20 to -70mv
What channels control the small repolarization in phase one
Ito channels
What potassium channels/currents are active in phase 2?
All (Ito, Ik, Ikl) but overpowered by Ca2+ influx and potential stays the same.
What channels are active in phase 3?
Most effect of Ik. All 3 (Ito, Ik, Ikl) to counteract Ca2+ influx and repolarize cell.
When are L Ca2+ channels open?
+10mv, during phase 0 of the fast fiber action potential, open rapidly but deactivate slowly
When are T Ca2+ channels open
-20mv, during phase 0 of the fast fiber action potential, before the L type
Which are the are the most abundant of the Ca++ channels?
L type
The — of Ca2+ balances out the — of K+ to maintain the membrane potential unchanged and cause the plateau phase of the fast fiber action potential
influx, efflux
What ends the plateau phase and begins repolarization?
The Ca++ channels close and K+ efflux predominates
What is the effect of calcium blockers (Diltiazem)?
L type
What is the effect of Diltiazem (calcium blocker)
Decreases plateau phase, lets K+ currents have an upper hand so that repolarization in phase 3 begins much earlier. Starts to make ventricle AP look like atrium.
Torsades de Pointes Phenomenon/Early After Depolarizations
Lack of initiation of phase 3 due to failure of calcium ions responsible for depolarization. Na and Ca channels are not slowed and depolarization is repeated without allowing K to flow out and repolarize. Need to shock.
What causes Early After Depolarization
Calcium continuously entering.
What are fast Na+ channels?
Phase 0 depolarization of non-pacemaker cardiac action potentials (Atria, ventricles, Purkinje)
What are slow Na+ channels?
“Funny” pacemaker current (If) in cardiac nodal tissue (SA, AV)











-
Physiology189
-
Physiology2125
-
Cardiac Physiology 342
-
Cardiac Physiology 440
-
Actin and Myosin19
-
Heart Failure38
-
Left-Right Shunt Congenital Heart Disease44
-
CV Pathology132
-
Renin-Angiotensin System62
-
Endocarditis43
-
Endothelium Function and Pathology (Brodsky)76
-
Congenital Heart Disease-Levitas69
-
Aortic Valve Stenosis-Merkin54
-
Acute Myocardial Infarction- Zahger135
-
Cardiovascular Noninvasive Imaging76
-
Chronic Angina46
-
Invasive Cardiology- Weinstein28
-
Acute Coronary Syndrome19
-
Mitral Valve Disease-Merkin50
-
Heart Failure Clinical Aspects-Weinstein50
-
Cardiac Surgery-Ishay42
-
Case Studies-Kimko21
-
Arrhythmias-Katz153
-
Cardiovascular Pharmacology Questions-Henkin99
-
Cardio PBL- Henkin20
-
Case Studies in Valve Diseases-Kobal12
-
Pericardial and Myocardial Cases-Henkin40
-
New Deck2
