Frank-Starling Graph
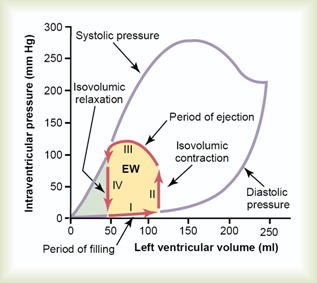
Diastolic response: length/volume vs pressure
There is little increase in pressure as the end-diastolic volume increases until the end (isometric contraction), at the end the fibers are all stretched out. Passive pressure since ventricle not contracting.
Systolic response: length/volume vs. pressure
Fast increase in pressure as volume decreases then levels off as fibers contract because the fibers are overextended at higher pressure. Then there is ejection and a decrease in pressure as the blood exits and the pressure is equalized to atrial pressure. The pressure is a measure of contractile force.
What is preload?
Increased length of fibers/ventricular wall stress/increased filling pressure of ventricles at end diastolic volume.
What is afterload?
Aortic pressure during ejection period/aortic valve opening. Resistance to what is being pushed out by the ventricle so afterload is inversely proportinoal to pressure in ventricles. Refers to the load that the perloaded muscle has to work against.
Laplace’s law and wall stress
WS=Pxr/(2*wall thickness) or σ = P.r/ 2h. Explains thickening of arteries and ventricles. Wall stress during systolic ejection is equivalent to the afterload. Pressure in equation can be estimated from arterial systolic pressure.
How does aortic diastolic pressure relate to the afterload?
Aortic pressure already exists (due to HTN, etc) even though valve hasn’t opened yet. Heart needs to pump harder to push blood against this resistance. A higher aortic pressure means more afterload.
What happens to pressure as afterload (aortic pressure) increases with preload constant?
Increases with constant slope until the pressure of the aorta is equal to that in the ventricle and there is no bloodflow–>heart failure. Essentially the effect of essential hypertension.
What happens to the pressure vs afterload graph with an increased preload?
Same graph but moved up, the left ventricular pressure developed at all points will increase and the new curve will be parallel and on top of the original one. Peak isometric force will be reached at a higher level and a change in peak isometric force versus initial fiber length (preload) will have occurred. NOT a change in contractility.
Contractility definition
Change in peak isometric force vs. initial fiber length (EDV). Intrinsic property of the cardiac cell that defines the amount of work that the heart can perform at a given load. Determined by availability of intracellular Ca2+.
Contractility in a normal heart vs Norepinephrine and Heart Failure (Graph)
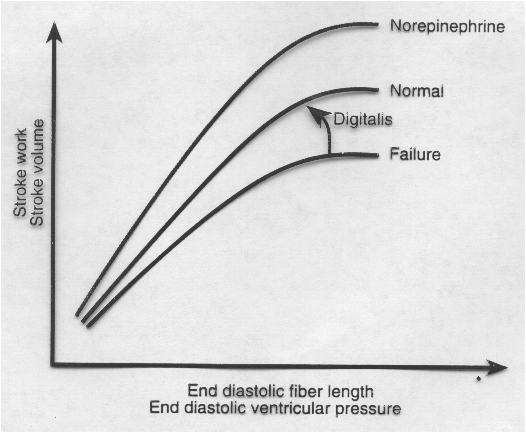
What is the effect of heart failure on pumping?
Decreases contractility, works with a higher preload due to a reduced ventricular ejection and high blood volume due to fluid retention.
How does diminished heart failure cause CHF?
HTN causes Back pressure in LA, into pulmonary vein, into lungs, fluid in lungs (alveoli), CHF
How does the change in left ventricular pressure over time change with failing heart or with epinephrine?
Epinephrine increases contractility and also ventricular pressure/instantaneous change in time. Failing heart has lower contractility and lower change in ventricular pressure/time.
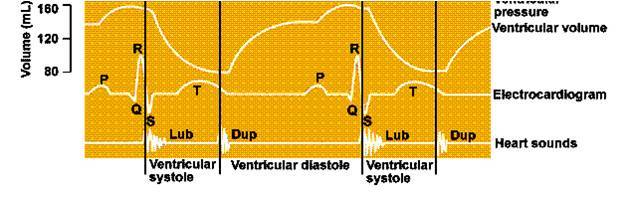
What is S1?
AV valves closing during early ventricular contraction
S2?
Semilunar valves closing during early ventricular relaxation
Heart sounds graph with time and ventricular phases
Mechanism of aortic stenosis
Pressure doesn’t rise high enough to open aortic valve all the way and valve is difficult to open because it’s hard. Ventricle contraction presses on aortic valve and aortic pressure will not rise with ventricular pressure.
What is the area under the pressure/volume loop?
Measure the work performed by the ventricle
Cardiac cycle beginning with mitral valve opening:
Mitral valve opening-filling-mitral valve closing-isovolumic contraction-aortic valve opening-rapid ejection phase-slow ejection phase-aortic valve closing-isovolumic relaxation-mitral valve opening
What happens if the afterload and contractility are constant but preload is increased (as in IV)?
Left ventricle EDV will rise, stroke volume will increase by Frank-Starling mechanism and ESV will be the same.
What is the effect of a hypertrophied ventricle on the pressure/volume curve?
Increases slope of diastolic filling curve, EDV is decreased. If afterload and contractility remain constant, SV is reduced.
What happens if the preload and contractility are kept constant but afterload is increased ( as in hypertension or aortic stenosis)?
Pressure generated by LV increases, more ventricular work is used to overcome resistance to ejection. Less fiber shortening takes place. Increased LV-ESV. Stroke volume is reduced.






-
Physiology189
-
Physiology2125
-
Cardiac Physiology 342
-
Cardiac Physiology 440
-
Actin and Myosin19
-
Heart Failure38
-
Left-Right Shunt Congenital Heart Disease44
-
CV Pathology132
-
Renin-Angiotensin System62
-
Endocarditis43
-
Endothelium Function and Pathology (Brodsky)76
-
Congenital Heart Disease-Levitas69
-
Aortic Valve Stenosis-Merkin54
-
Acute Myocardial Infarction- Zahger135
-
Cardiovascular Noninvasive Imaging76
-
Chronic Angina46
-
Invasive Cardiology- Weinstein28
-
Acute Coronary Syndrome19
-
Mitral Valve Disease-Merkin50
-
Heart Failure Clinical Aspects-Weinstein50
-
Cardiac Surgery-Ishay42
-
Case Studies-Kimko21
-
Arrhythmias-Katz153
-
Cardiovascular Pharmacology Questions-Henkin99
-
Cardio PBL- Henkin20
-
Case Studies in Valve Diseases-Kobal12
-
Pericardial and Myocardial Cases-Henkin40
-
New Deck2
