1) A patient with apparent symptoms of hypothyroidism. What laboratory tests would be the most appropriate to perform?
- *Measure the free T3 / T4 levels.**
- *Measure TSH levels** and see if they are proportional to the TH levels. If the levels are low this could indicate a secondary or teriary hypofunction (though tertiary is very rare), and if the levels are high, this could indicate a primary hypofunction (thyroid damage, especially of autoimmune diseases). Check for antibodies against autoimmune diseases.
2) A 40 year old woman seeks evaluation for subfebrility and diarrhea commenced 2–3 weeks before. Blood glucose: 6.6 mmol/l. Blood pressure: 160/85 mmHg, heart rate: 120/min. Serum TSH: 0.15 mU/l (decreased), FT4: 60 pmol/l (elevated), TRAb titer elevated, TPO-antibody positive.
What is the most likely diagnosis? What other test would you order to specify your diagnosis?
Autoimmune TSH receptor activating thyroiditis, causing hyperthyroidism. BUT, it also has TPO-antibodies. These will eventually cause the thyroid destruction. This is the initial stage of Hashimoto thyroiditis. Basedow-Graves disease has no TPO-Ab!!
Graves disease has TSH receptor activating and TSH receptor inhibiting andtibodies, but no thyroperoxidase antibodies.
Tests: Perform a second random blood glucose test and perhaps a oGTT to rule out DM.
A 42 year old woman developed diffusely enlarged, painless thyroid glands. Total T4 is decreased, thyroid uptake of radioiodine is low. ECG reveals low voltage and bradycardia. The thyroid autoimmunity panel demonstrates the presence of TgAb and TPO-Ab. What is the most likely diagnosis? Is this condition characterized by a hypo or hyperfunction of the thyroid gland?
Conclusion: diffuse goiter caused by end stage Hashimoto Thyroiditis. This is a hypothyroidism caused by Hashimoto thyroiditis (autoimmune destruction of thyroid gland). At the beginning of the disease ther are high amounts of stored hormone released → increased serum levels → degredation → no thyroid hormone can be produced → hypofunction develops.
4) A schoolgirl at the age of 14 without any complaints develops diffusely enlarged painless thyroid glands recognized accidentally by the school doctor. Laboratory findings: FT4 is slightly decreased, whereas total T3 is slightly elevated. Thyroid uptake of radioiodine is increased. FT4 gets normalized after treatment with anorganic iodine.
What is the most likely diagnosis? Try to interpret the opposite changes in hormone levels.
This patient has iodine deficiency. Without iodine, the thyroid glands cannot produce thyroid hormones, which means there is no negative inhibition of TSH. TSH will overstimulate the thyroid gland, to try and increase thyroid hormone production, which causes the goiter.
Treatment: Try to promote T3 production (has one less iodine but is more potent).
Iodine deficiency is rare in developed countries, because it is put into our salt. It is still possible to be found with puberty, pregnancy or underdeveloped countries.
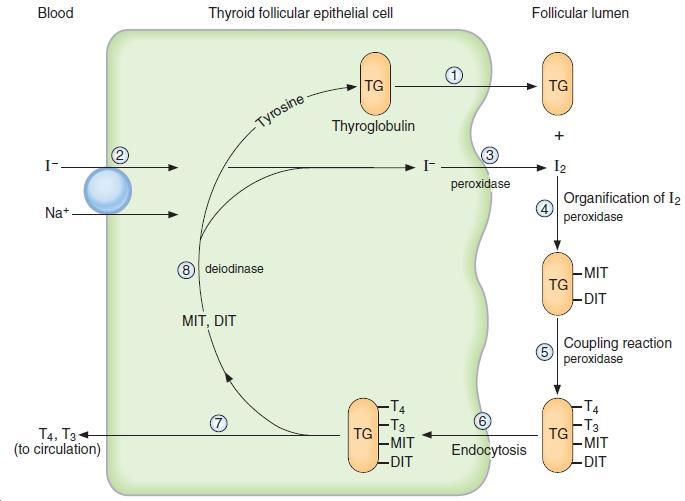
5) An 11 month old baby with protruded belly and retarded in movement development has been brought for medical evaluation. Serum FT4 and FT3 are decreased. Serum MIT/DIT are elevated and their urinary excretion increased.
What is the most likely diagnosis?
MIT and DIT are mono-iodinated Tyrosine and di-iodinated Tyrosine.
Congenital hypothyroidism,
Probably due to a congenital enzyme deficiency involved in incorporating MIT and DIT together into TH3/4 or onto Thyroglobulin. TH.
6) List those thyroid tests that are considered helpful in the diagnosis of thyroid cancer!
- Fine needle biopsy: histological / cytological exam (best)
- Radioactive scintigraphy: (cold nodule shows there is no activity in the thyroid glands) Iodine-131 scintigraphy is used in whole body screening for metastic thyroid cancer.
- Thyroid ultrasound: used to distinguish solid from cystic (seldom malignant).
- Measure the serum level of calcium and calcitonin. If there is hypocalcemia and increased calcitonin, it can be indicative of medullary thyroid carcinoma (of the c-cells).
- Check tumor markers for thyroid cancer
- Measure thyroglobulin concentration in plasma: if it is present, it is an indication of cancer / inflammation
-
Week 1 Inflammation42
-
Week 2 Heart Failure21
-
Week 3, Arrhythmias16
-
Week 3, Coronary heart disease15
-
ECG: Arrhythmias6
-
Hematology reference values14
-
Blood ion reference values7
-
Blood metabolites and proteins reference values10
-
Renal function and urine Reference parameters6
-
ECG reference values4
-
Semifinal review random cards4
-
Hypertension reference values5
-
BMI, malnutrition, obesity, hyperlipidemia reference values3
-
Diabetes4
-
Hyperlipidemia Reference values10
-
Pathophys lab questions and answers14
-
Lipid lab diagnositcs questions5
-
Hepatobiliary lab diagnostics10
-
Blood bilirubin and liver protein reference values5
-
GI Lab diagnostics questions7
-
Hypothalamic Pituitary Lab Diagnositcs7
-
Gonads and reproductive disorder lab diagnostics3
-
Thyroid disorders lab diagnositcs6
-
Adrenal gland lab diagnostics12
