What are the presenting features of GORD?
Examination is remarkable
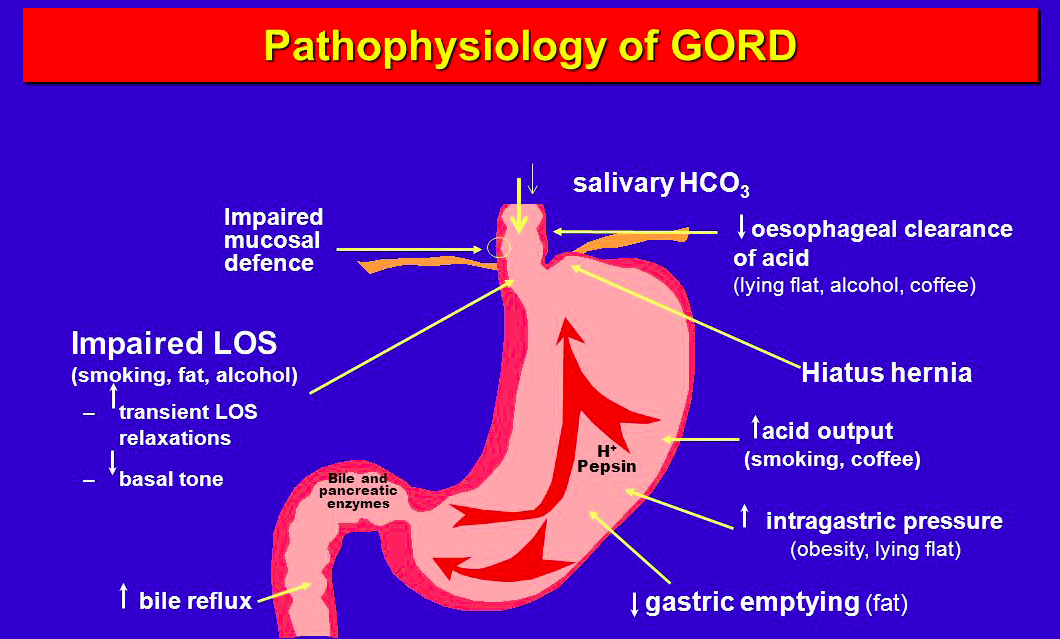
- Retrosternal burning chest/epigastric pain that is worse when lying down, after meals, bending over or straining.
- Excessive belching
- Odynophagia
- Chronic/Nocturnal cough
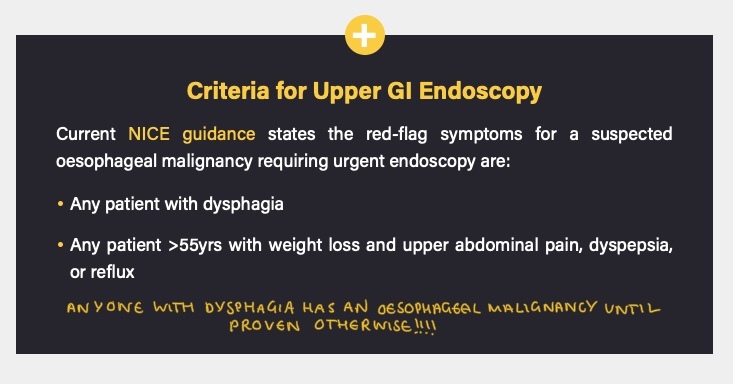
What are some red flag features you should check for that could indicate a GI malignancy when a person presents with GORD symptoms?
- Dysphagia
- Weight loss
- Early sateity
- Malaise
- Loss of appetite
What are some risk factors for GORD?
- Male
- Age
- Obese
- Smoking
- Alcohol
- Caffeine
- Spicy foods
- Fatty processed foods

What are some differentials for GORD?
- Oesophageal or gastric malignancy
- Peptic ulcer
- Oesophageal motility disorders
- Oesophagitis
- Consider cardiac and biliary disease
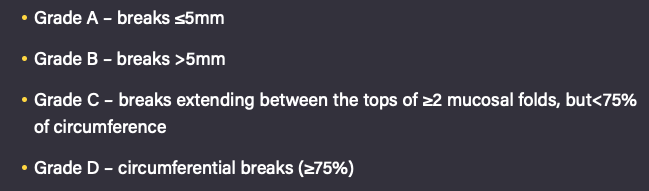
What is the LA classification of GORD?
- Grades reflux oesophagitis based on severity from the endoscopic findings of mucosal breaks in the distal oesophagus.
- Grade A-D (see image)
- Grade B does not extend over the tops of 2 mucosal folds
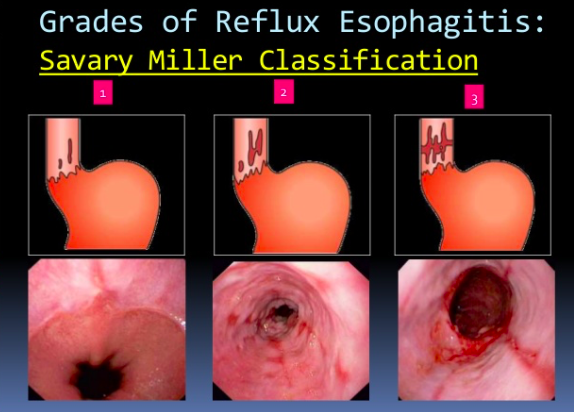
What is the Savary Miller Grading of GORD?
1 - Single/Multiple erosions on a single fold
2 - Multiple erosions on multiple folds
3 - Multiple circumferential erosions
4 - Ulcer/Stenosis/Shortening
5 - Barrett’s Oesophagus
What investigations are done to confirm a diangosis of GORD?
- Usually a Hx and resolution with PPI is enough
- May do endoscopy if suspect malignancy (dysphagia or >55 with alarm symptoms) or complications
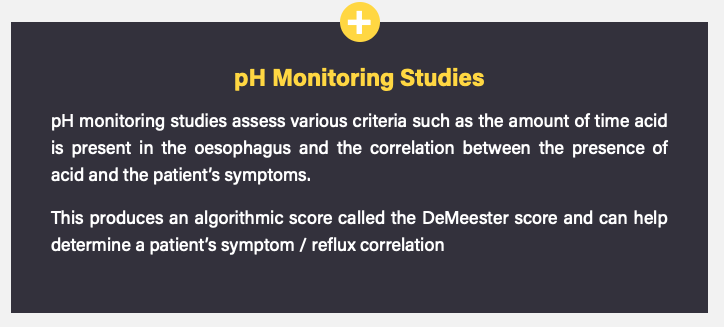
- Gold standard: 24h pH monitoring combined with oesophageal manometry to exclude oesophageal dysmotility. Used when medical treatment fails and surgery is being considered
What are the main indications for surgical management of GORD?
- Failure to respond to medical therapy
- Patient preference to avoid life-long medication
- Patients with complications of GORD (especially respiratory complications such as recurrent pneumonia or bronchiectasis)
What are the different surgical options for the treatment of GORD?
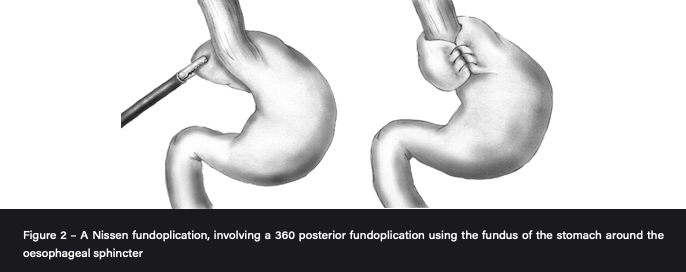
- Nissens Fundoplication: fundus wrapped around GOJ to mimic LOS laparoscopically.
- Stretta: radio-frequency energy delivered endoscopically to thicken LOS
- Linx®: string of magnetic beads to tighten LOS
What are the main post op complications of fundoplication?
- Dysphagia (if too tight)
- Bloating
- Inability to vomit/belch (Gas-Bloat syndrome)
- New onset diarrhoea
Most s/e settle after 6 weeks

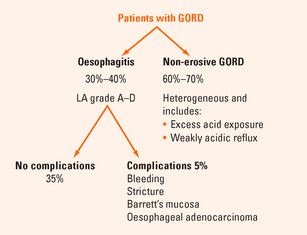
What are some of the complications of GORD?
- Aspiration pneumonia
- Barrett’s oesophagus (Fundoplication does not lower risk of this developing into cancer)
- Oesophagitis
- Oesophageal strictures
- Oesophageal cancer
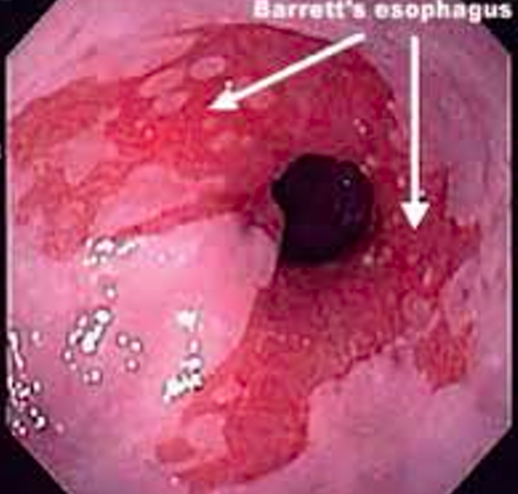
What is the pathophysiology of Barret’s oesophagus and how does it present?
- Metaplasia of the lower oesophagus from stratified squamous to simple columnar
- History of chronic GORD symptoms with remarkable exam
- Same risk factors as for GORD plus >50, FHx, caucasian, hiatal hernia
How do you investigate and diagnose a suspected case of Barrett’s oesophagus?
- Histologically by taking a biopsy during OGD for chronic or resistant GORD
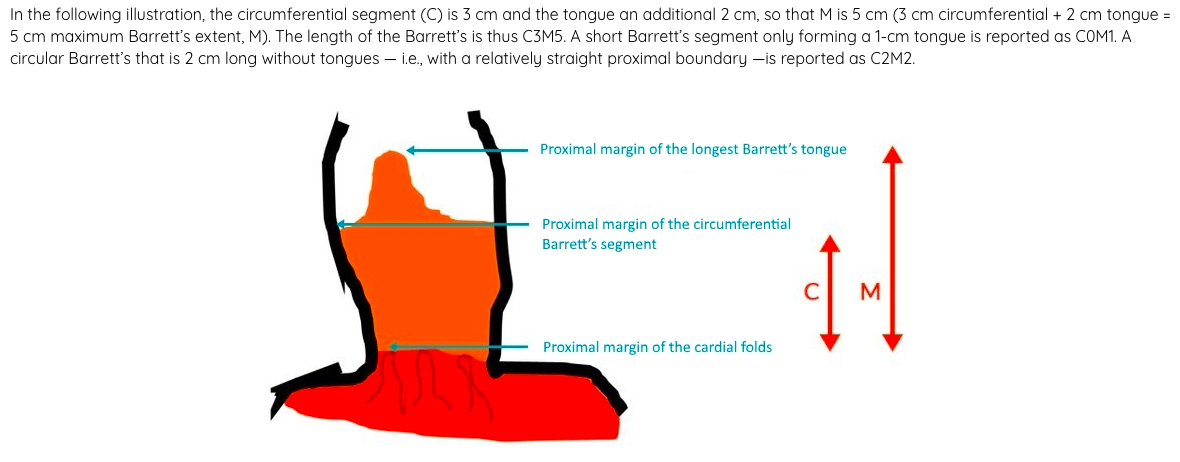
- Severity depends on amount of dysplasia and the length (Prague classification)
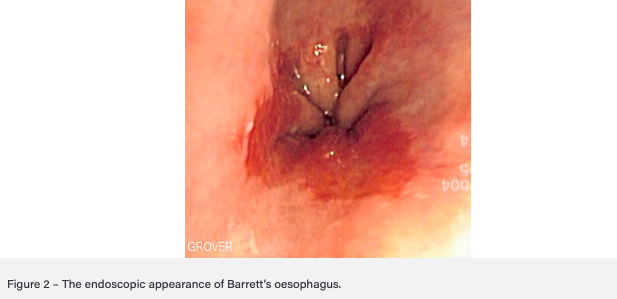
- On endoscopy will look red and velvety with some preserved pale squamous islands
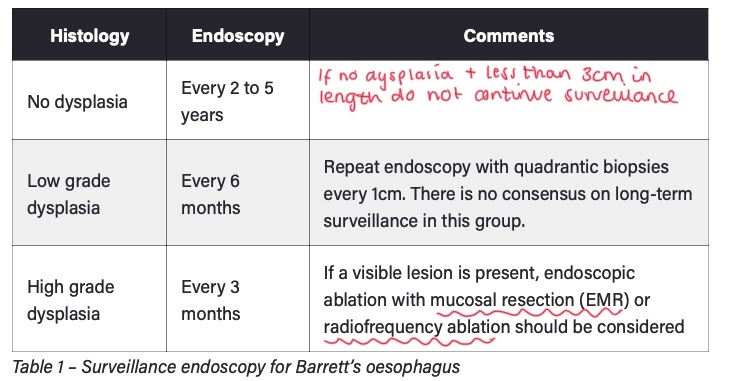
How is Barrett’s oesophagus managed?
- High dose PPI BD
- Lifestyle advice to reduce triggers and stop any drugs that will worsen e.g NSAIDs
- Monitor for progression to adenocarcinoma with regular endoscopy. If high grade dysplasia do EMR/ESR or Radiofrequency ablation
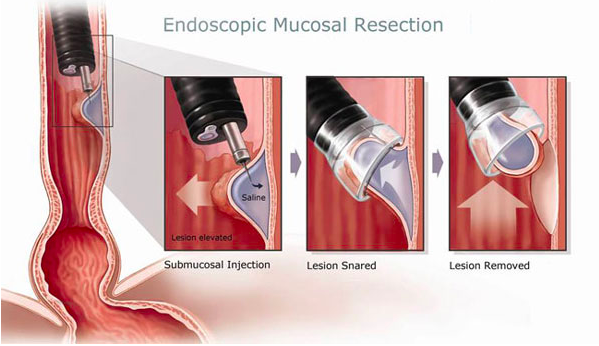
When there is high grade dysplasia in Barrett’s oesophagus, what should be the course of action?
High risk of progressing to cancer so should be resected with endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD).
Adenocarcinomas on routine screening for Barrett’s Oesophagus tend to be early stage and have a better prognosis than those found outside of screening
What are the histological types of oesophageal cancer and what is their typical location?
Squamous Cell Carcinoma: middle and upper thirds
Adenocarcinoma: lower third due to metaplastic change then dysplasia then malignancy
Rare: leiomyosarcoma, rhabdomyosarcoma, lymphoma
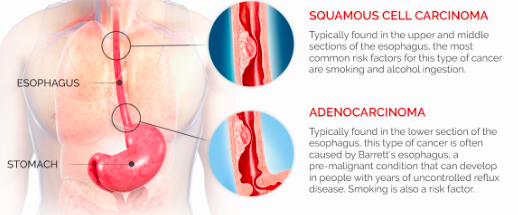
What are the risk factors for developing each histological type of oesophageal cancer?
SCC: developing world, smoking, excess alcohol consumption, chronic achalasia, Vit A deficiency, Fe deficiency
Adenocarcinoma: long standing GORD, obesity, high fat intake, Barrett’s
What are some clinical features of oesophageal cancer?
Early on vague symptoms which is why it is caught late. Red flags in bold
- Progressive dysphagia, firstly solids then liquids
- Significant weight loss due to anorexia and dysphagia
- Odynophagia
- Hoarseness
- Supraclavicular lymphadenopathy
- Metastatic signs (jaundice, hepatomegaly, ascites)
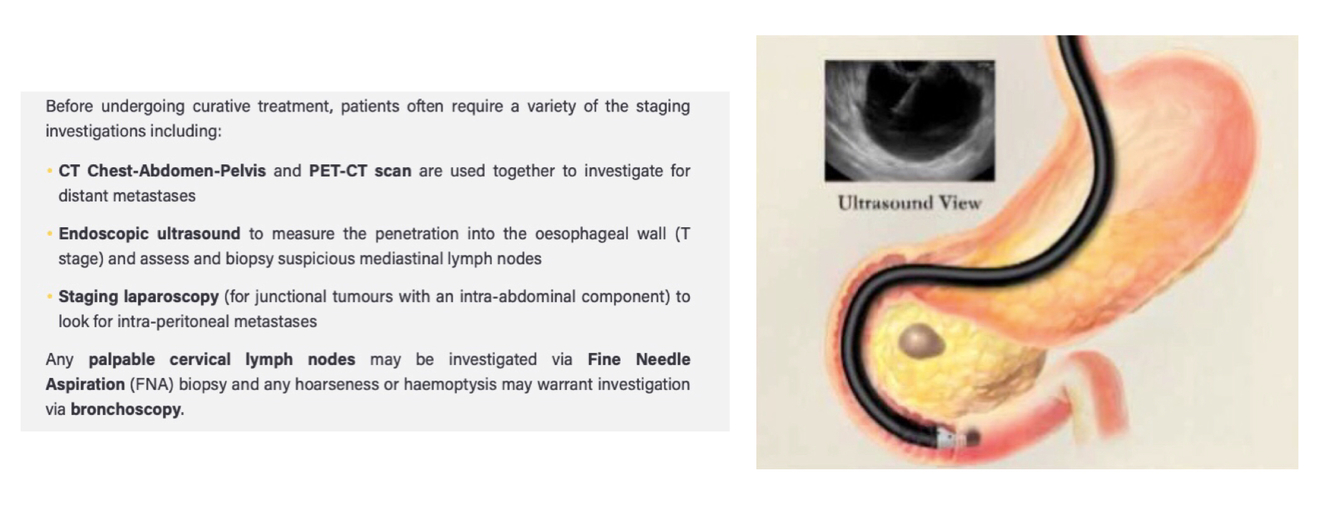
What is the initial and subsequent investigations for a suspected oesophageal malignancy?
- Upper GI Endoscopy (OGD) and biopsy within 2 weeks
- Then see image
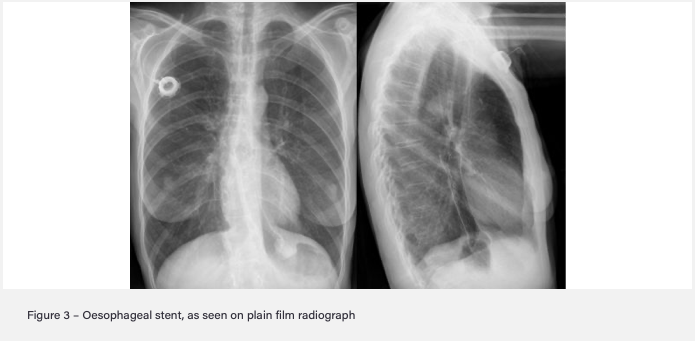
Oesophageal cancer often presents at a late stage so around 70% of patients are treated palliatively. What are some palliative treatment options for this?
- Oesophageal stent if difficulty swallowing
- Radio/Chemo to shrink tumour and improve symptoms
- Thickened fluid and nutritional supplements
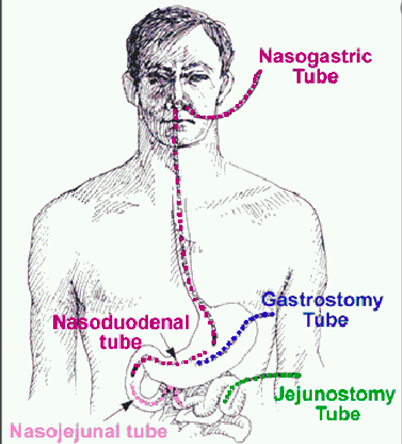
- Radiologically-Inserted Gastrostomy (RIG) tube if severe dysphagia so cannot tolerate enteral feeds
What is the prognosis for oesophageal cancer?
- Poor 5 year survival of 5-10% as presents so late
- Median survival for palliative is 4 months
- 60% 5 year survival if surgically treated
What is the curative management for oesophageal cancer if the cancer is not too advanced?
- Usually surgical with/without neoadjuvant chemoradio/chemo.
- If early cancer/high grade Barrett’s then EMR
SCC: usually in upper oesophagus so difficult to operate on so chemo-radiotherapy
Adenocarcinoma: neoadjuvant chemoradiotherapy/chemotherapy followed by surgical oesophageal resection
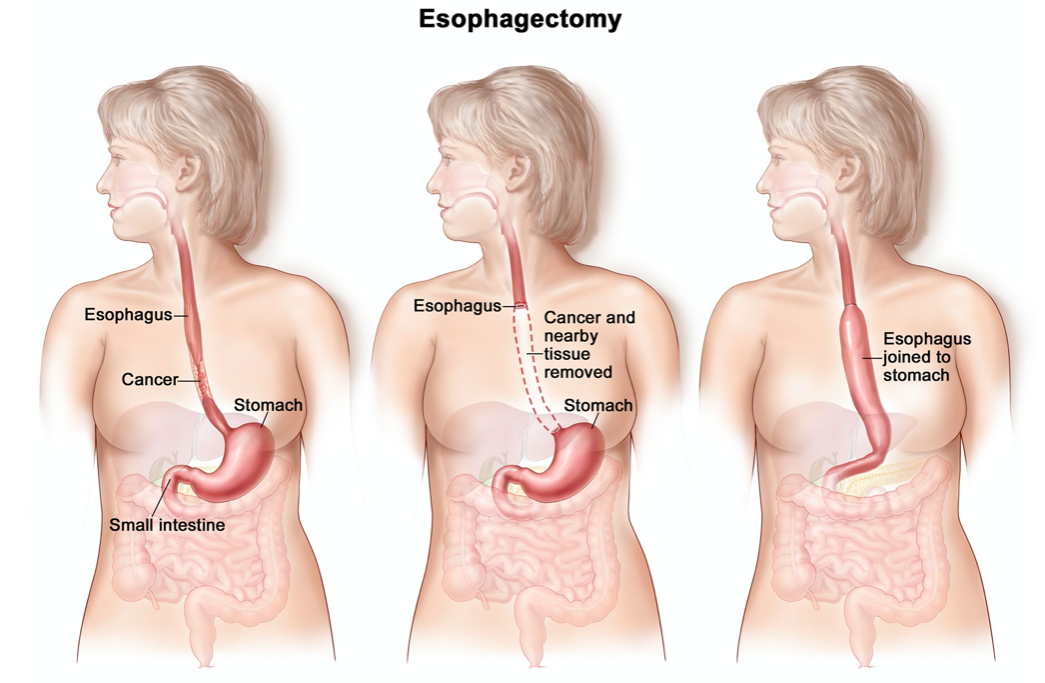
What are the main complications of an oesophagectomy used to treat oesophageal cancer?
- Pneumonia (most common)
- Anastomotic leak!!! (any deterioration in oesophagectomy patient is leak until proven otherwise)
- Death
- Post operative nutrition issues (lose reservoir capacity of stomach so need feeding jejunostomy or small frequent meals)
Why is surgical treatment for oesophageal cancer considered a major high risk surgery?
- Both the abdominal and chest cavities need to be open
- One lung is deflated for up to 2 hours
- 30 day mortality up to 4%
- Takes patients 6-9 months to fully recover





























































-
1 - Care of the Surgical Patient123
-
2 - General and T&O Imaging72
-
3 - GI Presentations100
-
4 - Upper GI92
-
5 - Hepatobiliary122
-
6 - Lower GI126
-
7 - Anorectal40
-
8 - Breast68
-
9 - KUB77
-
10 - Prostate and Genital Tract82
-
11 - T&O General Principles67
-
12 - T&O Spine, Hip and Thigh89
-
13 - T&O Knee and Leg42
-
14 - T&O Ankle and Foot53
-
15 - T&O Shoulder and Arm57
-
16 - T&O Elbow and Forearm39
-
17 - T&O Wrist and Hand44
-
18 - Peripheral and Arterial Vascular Disease116
-
19 - Vascular64
-
20 - Perioperative Care102
-
21 - Perioperative Care 286
