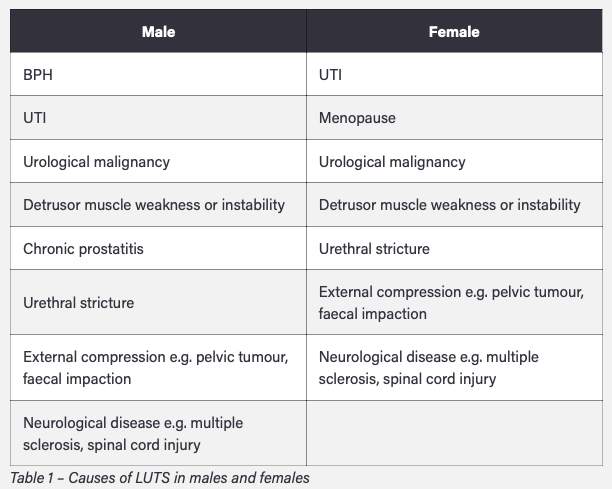
What is the aetiology of LUTS in men and women?
Most common:
Men: BPE (BPH)
Women: UTI
Drinking fluids late at night, excess alcohol intake, and excess caffeine intake can exacerbate LUTS. Polyuria caused by T2DM can mimic LUTS
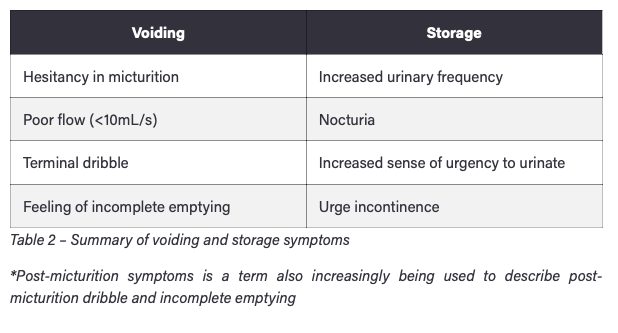
How can LUTS be categorised?
What are some important questions/examinations to do when a patient presents with LUTS?
- Associated symptoms: visible haematuria, suprapubic discomfort, or colicky pain
- DHx: anticholinergics, antihistamines, bronchodilators are known to exacerbate LUTS
- Consider DRE and examination of external genitalia
- IPSS score
What are some investigations done when patients present with LUTS?
Initial
- Urinalysis and culture
- Urinary frequency and volume chart
- Post-bladder scanning and flow rate
- Bloods (FBC, U+E’s, PSA)
Specialist
- Gold standard is Cystoscopy and used if recurrent infection or haematuria
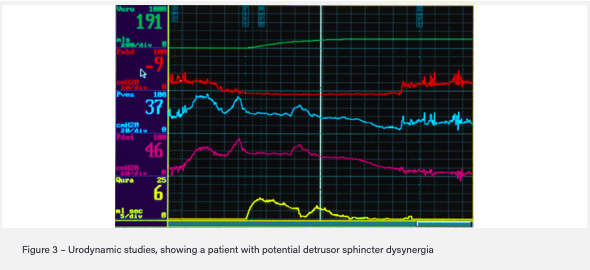
- Urodynamic studies to look at flow rate, detrusor pressure
- Upper urinary tract imaging, such as via ultrasound or CT scanning
How are people with LUTS managed conservatively and pharmacologically, apart from treating the underlying cause?
Conservatively
- Regulate fluid intake, alcohol and caffeine
- Urethral milking and double voiding
- Pelvic floor exercises
- Bladder training techniques
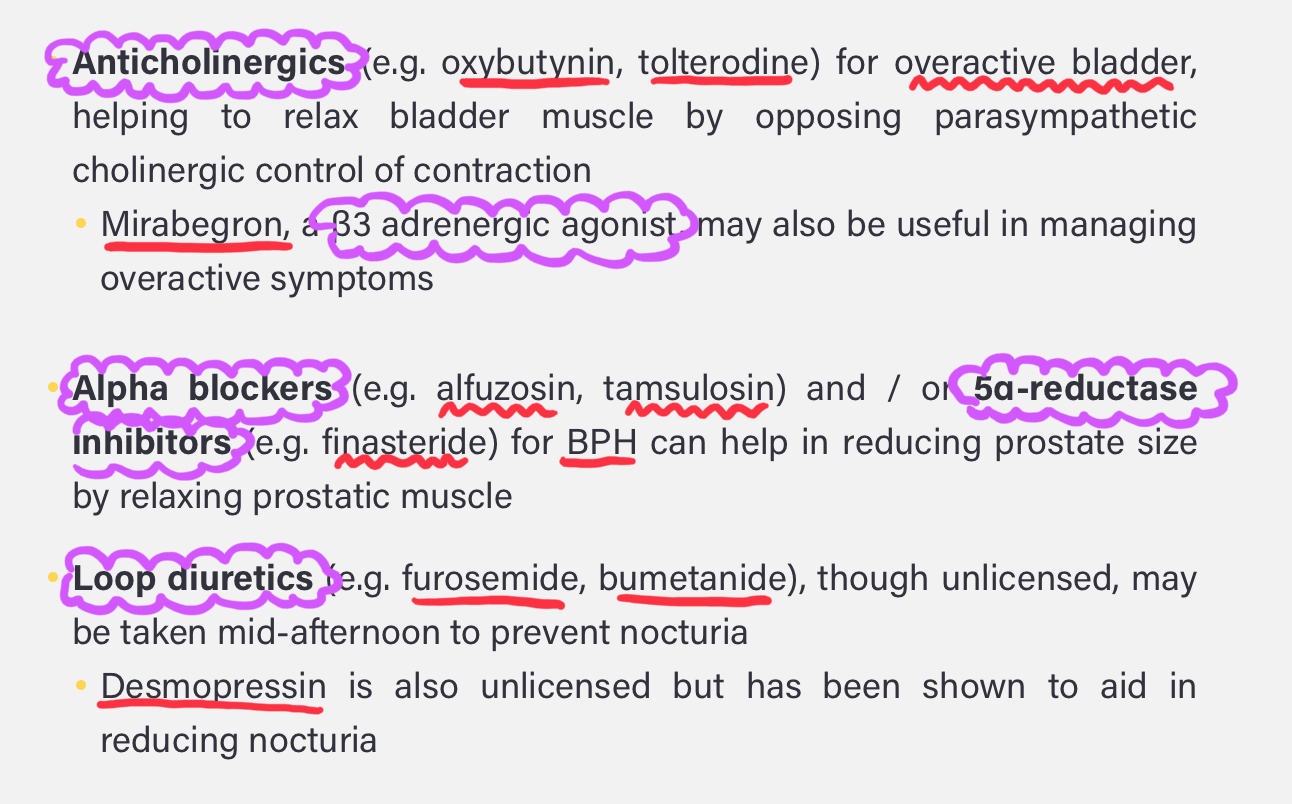
Pharmacologically
- Alpha blockers
- B3 agonists
- Anticholinergics
- Loop diuretics
What are some complications of leaving LUTS untreated?
- Risk of infection
- Renal and bladder calculi due to stagnation
- Overflow incontinence if chronic obstruction
- Renal failure
- Bilateral hydronephrosis
- Acute renal failure with BPH
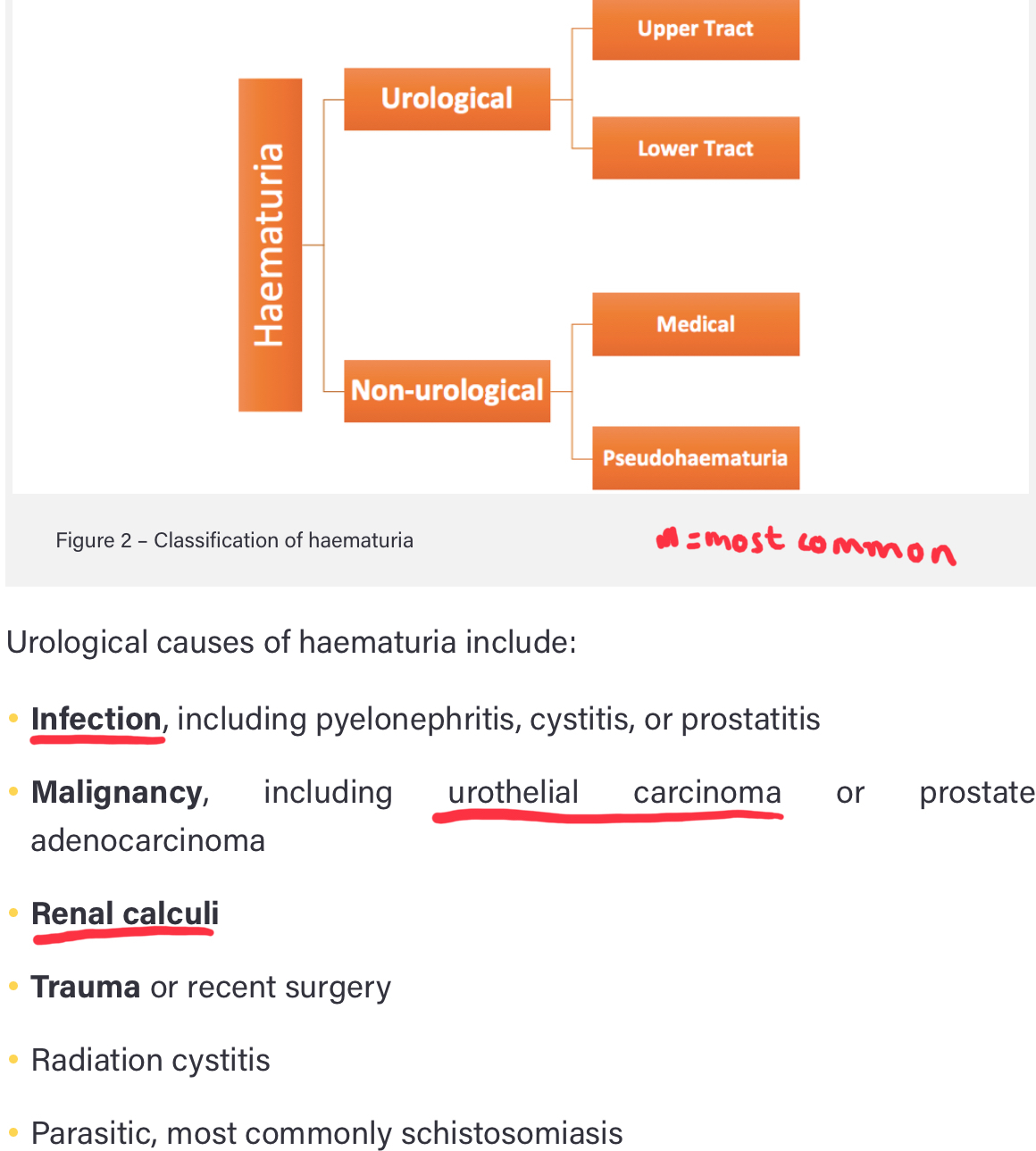
How can haematuria be classified and what is the aetiology?
- Visible (VH) OR
- Non visible (a-NVH/s-NVH): symptomatic or asymptomatic OR
- Pseudohaematuria: foods like beetroot, medication (such as rifampicin or methyldopa), hyperbilirubinuria, myoglobinuria
- BPH can also cause haematuria
What questions do you need to ask in a history with someone presenting with haematuria?
- Timing:* if total suggests bladder or upper tract source, if terminal then severe bladder irritation
- Recent trauma*
- DHx*
- Smoking status* (urological cancer)
- Exposure to industrial dyes* (bladder cancer)
- Travel history* (Schistosomiasis)
Abdominal exam, possible DRE and possible genital exam
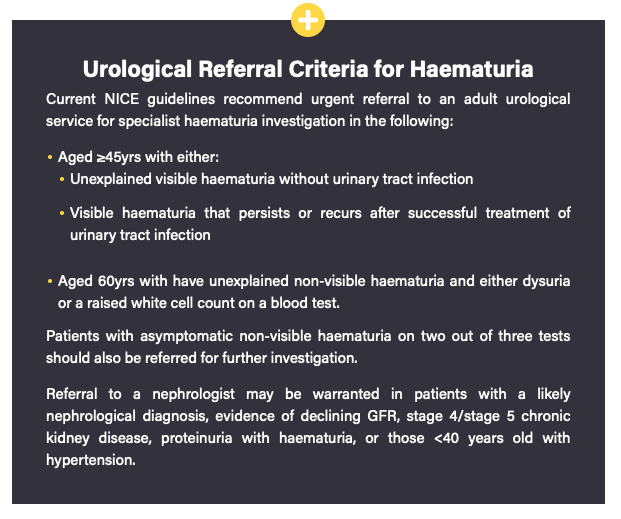
How are patients with haematuria investigated?
Initial
- Urinalysis (check for nitrates/leucocytes to indicate infection. Trace blood not haematuria, needs to be >1+)
- Baseline bloods (FBC, U+E’s, Clotting)
- PSA after counselling
- If deranged renal function take ACR
- Refer to specialists
Specialist Ix
- Flexible cystoscopy is gold standard
- Urine cytology
- US KUB imaging for NVH
- CT Urogram for VH
What is acute urinary retention and the aetiology of this?
New onset inability to pass urine which leads to pain and discomfort with significant residual volumes
Most common cause: BPH
Obstructive causes: urethral stricture, prostate cancer, constipation, UTIs
Medication: antimuscarinics, spinal anaesthesia
Neurological: severe pain, peripheral neuropathy, iatrogenic nerve damage during pelvic surgery, UMN disease (MS, Parkinson’), Bladder Sphincter Dysinergy
What are the clinical features of acute urinary retention?
- Acute suprapubic pain
- Inability to micturate
- Palpable distended bladder with tenderness
- Acute confusion in the elderly
Do PR to rule out constipation and prostate pathology

What are some investigations that are done when acute urinary retention is suspected?
- PR/PV exam
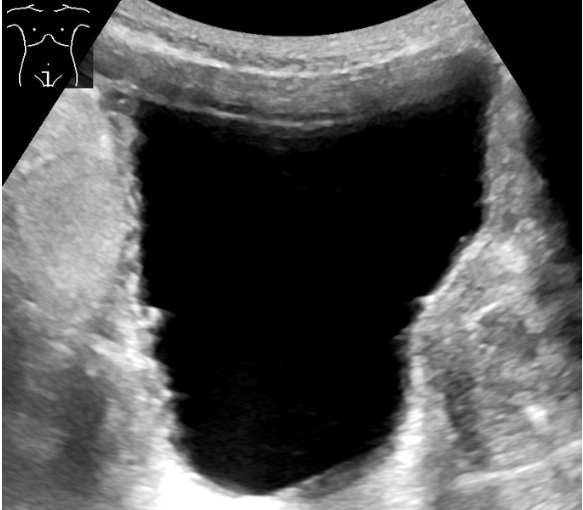
-Post-void bedside bladder scan
- Post catheterisation CSU/MSU
- Routine bloods (FBC, U+E’s, CRP)
- US KUB scan if suspect high pressure retention to look for hydronephrosis
- Monitor for post-obstructive diuresis
How is acute urinary retention managed?
- Immediate catheterisation and measure residual volume
- Treat underlying cause e.g Tamsulosin for BPH
- Check CSU for infection and review meds to see if there was a cause
- If large retention volume (>1000ml) monitor for post-obstructive diuresis
How long should a catheter be left in place after an episode of acute urinary retention and what complications would occur if they had not been treated with catheterisation?
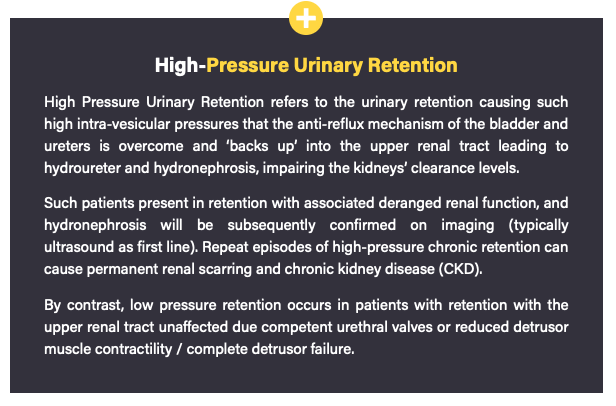
- High-pressure urinary retention: keep in place until definitive treatment (e.g TURP) to prevent further rentions that could cause an AKI and eventually CKD
- No evidence of renal impairment: TWOC 24-48 hours after insertion. If unsuccessful try again in TWOC clinic after longer interval. If mutiple failed attempts long term catheter until definitive treatment
Complication: AKI, CKD, renal scarring, UTI, renal stones due to stasis
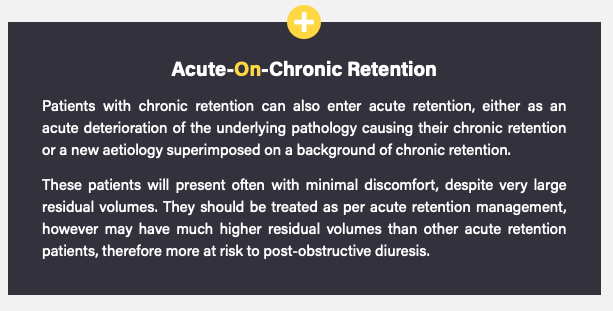
What is the pathophysiology of chronic urinary retention?
Most common in men: BPH
Most common in women: pelvic prolapse (such as cystocele, rectocele, or uterine prolapse)
Other: urethral strictures, prostate cancer, pelvic masses (fibroids), peripheral neuropathies, UMN diseases (MS)
How does chronic urinary retention present?
- Painless urinary retention
- Palpable distended bladder that is NOT tender
- Voiding LUTS e.g hesitancy, weak stream
- Overflow incontinence
- Nocturnal enurisis
Do DRE to check for prostate enlargement
How is chronic urinary retention investigated and managed?
Ix
- Post-void bedside bladder scan to look at retained urine
- Routine bloods (FBC, U+E’s, CRP)
- US KUB if high-pressure retention to look for hydronephrosis
Mx
- Treat underlying cause, catheterise if >1000ml residual whilst waiting for treatment
- Long term catheter/ICS with monitoring for post obstructive diuresis
- NO TWOC as concerns of repeat renal injury
What are the complications of chronic urinary retention?
- UTI
- Bladder calculi
- CKD if repeated episodes

What are the different compositions of renal tract stones (kidney and ureter stones)?
More common in males <65
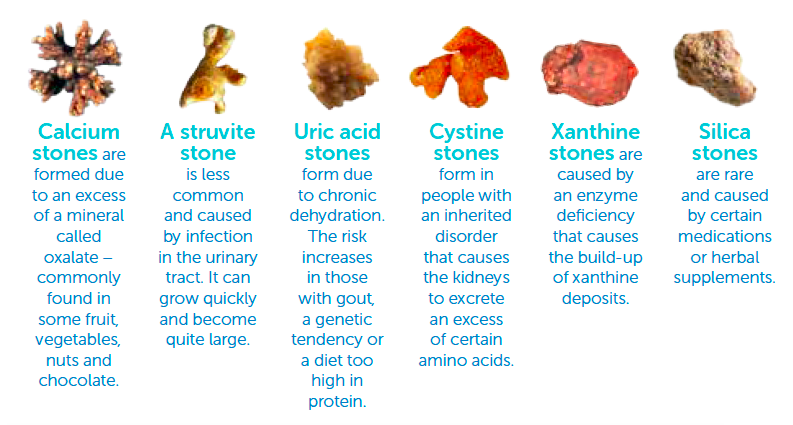
- Calcium (80%): calcium oxalate (35%), calcium phosphate (10%), or mixed oxalate and phosphate (35%)
- Struvite: magnesium ammonium phosphate, cause staghorns
- Urate: only radiolucent stones
- Cystine
What is the pathophysiology of renal tract stones?
Oversaturation in the urine
Cystine: homocystinuria affects the absorption and transport of cystine in the bowel and kidneys so builds up
Urate: high levels of purine in the blood, from diet (e.g. red meats) or through haematological disorders (such as myeloproliferative disease)
Hypocitraturia: citrate is a stone inhibitor so less of it causes stoens to form
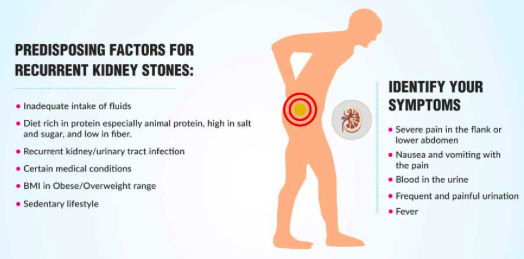
What are the clinical features of renal calculi and what are some differential diagnoses?
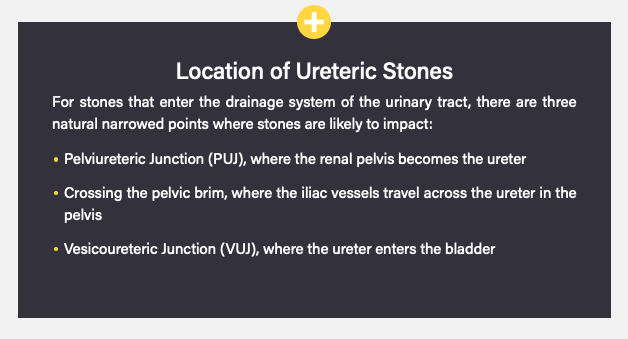
- Sudden onset one sided severe pain radiating from flank to pelvis (loin to groin ureteric colic) due to increased peristalsis around obstruction
- N+V
- Haematuria (usually non-visible)
- May have fever, rigors or lethargy if associated with infection (CONSIDER SEPSIS)
- Exam usually remarkable, may be some flank/renal angle tenderness but no suprapubic tenderness
DD: pyelonephritis, ruptured AAA, biliary pathology, bowel obstructon, MSK pain, lower lobe pneumonia
How are suspected renal calculi investigated?
- Urine dip and culture (microscopic haematuria)
- Routine bloods (FBC, CRP, U+Es, Urate, Ca)
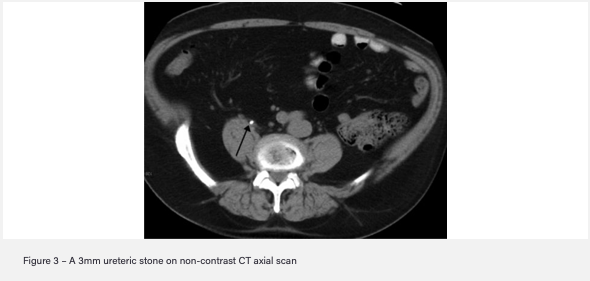
- Gold standard imaging: Non-contrast CT KUB
- Other imaging: AXR with IV urogram (most stones not radiolucent and high radiation exposure) or US to assess for hydronephrosis
How are renal calculi managed initially after diagnosis on investigation before definitive management?
Initial
- IV fluid resus as lot of vomiting and reduced fluid intake
- Sufficient analgesia (opioids or PR NSAIDs)
- IV abx and urology referral if suspect sepsis
- JJ stent or Nephrostomy immediately if obstructive nephropathy causing renal damage (infection and obstruction)
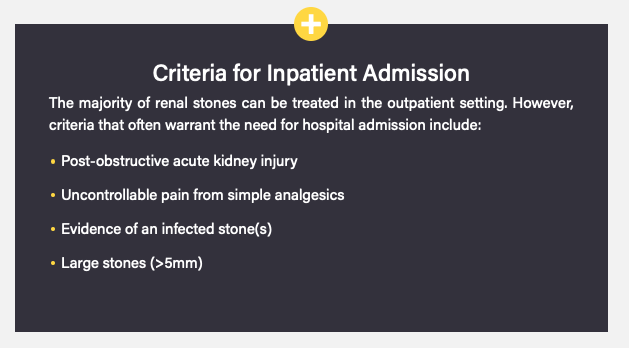
How are renal calculi managed definitively if they are over 5mm so cannot be passed spontaneously with hydration and analgesia?
Extracorporeal Shock Wave Lithotripsy (ESWL): sonic waves break up then pass spontaneously. Used for small stones and radiological guidance. Contraindicated in pregnancy or a stone over a bony landmark e.g pelvis
Percutaneous nephrolithotomy (PCNL): large and staghorn calculi. Percutaneous access then nephroscope put into renal pelvis and stones fragmented by lithotripsy
Flexible uretero-renoscopy (URS): passing a scope retrograde up into the ureter, fragmented through laser lithotripsy and the fragments subsequently removed

































-
1 - Care of the Surgical Patient123
-
2 - General and T&O Imaging72
-
3 - GI Presentations100
-
4 - Upper GI92
-
5 - Hepatobiliary122
-
6 - Lower GI126
-
7 - Anorectal40
-
8 - Breast68
-
9 - KUB77
-
10 - Prostate and Genital Tract82
-
11 - T&O General Principles67
-
12 - T&O Spine, Hip and Thigh89
-
13 - T&O Knee and Leg42
-
14 - T&O Ankle and Foot53
-
15 - T&O Shoulder and Arm57
-
16 - T&O Elbow and Forearm39
-
17 - T&O Wrist and Hand44
-
18 - Peripheral and Arterial Vascular Disease116
-
19 - Vascular64
-
20 - Perioperative Care102
-
21 - Perioperative Care 286
