What are the components of the Cardiovascular System?
- Pump - the heart
- Distribution system - vessels and blood
- Exchange mechanism - capillaries
- Flow control - arterioles and pre-capillary sphincters (resistance vessels)
- Capacitance - veins
How does Exchange of substancs between the blood and cells of the body occur?
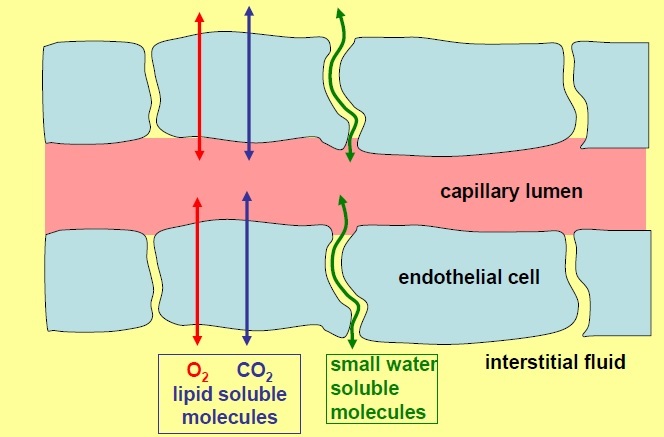
98% of exchange is by diffusion.
- Capillaries are composed of a single layer of endothelial cells surrounded by basal lamina.
- Lipophilic molecules such as O2 and CO2 can diffuse directly through the lipid blayer
- Small, hydrophilic molecules such as glucose, amino acids and lactate diffuse through small pores between endothelial cells.
- All molecules will move down their concentration gradient
What does the rate of diffusion depend on?
- Area
- Diffusion Resistance
- Concentration Gradient (difference)
Explain how the rate of diffusion depends on the area available for exchange
- The larger the area, the faster the rate of diffusion
- Area for exchange between capillaries and tissues is generally very large - depends on CAPILLRY DENSITY (number of capillaries per unit volume)
- A tissue which is more metabolically active will have more capillaries.
- Not all capillaries are always perfused so it represents the maximum area for exchange
- Generally, however, area is not limiting factor
Explain how the rate of diffusion depends on the diffusion resistance
the difficulty of movement through the barrier. Depends on:
- Nature of the molecule: hydrophilic or lipohilic, size (small hydropilic molecules can diffuse readily through pores, large hydrohilic molecules may be too big)
- Nature of the barrier: e.g.pore size and number of pores for hydropilic substances (some tissues have more or larger pores). Tight junctions e.g. in the brain decreases pore size which limits diffusion.
- Path length (depends on capillary density; path is shortest in the most active tisssues (highest capillary density)
- Diffusion resistance is mostly low - not generally the limiting factor.
Explain how the rate of diffusion depends on the concentration gradient
- The greater the concentration gradient, the greater the rate of diffusion
- The concentration which matters is between capillary blood and tissues
- FOr exchange to continue, the concentration gradient between the capillary blood and tissues must be maintained.
- Unless blood is supplied at an appropiate rate, the gradients driving exchange will dissipate and the nutrients will not be supplied at the right rate.
- A substance which is used by the tissues will have a lower concentration in capillary blood than arterial blood e.g. O2. How much lower depends on RATE tissues use the substance (causes [O2] drop) and RATE of blood through the capillary bed (if blood flow is fast, [O2] is maintained)
What does the suply of materials to the tissues depend most critically on?
- Concentration gradients driving xchange
- If all other things are equal, the supply of nutrient to a tissue depends most crtically on maintaining the right FLOW of bloodfor the prevailing level of metabolic activity. The CVS must maintain appropriate flows through ALL tissues.
What is the rate of blood flow also known as?
The perfusion rate which can be constant or vary enormously.
Describe the blood flow to the Brain
Metabolic needs are constant and can be met by a flow of 0.5ml/min/g
Th brain is extremely intolerant of flow interruption - blood flow is high and constant - 750ml/minute
Describe the blood flow to the heart
- At rest the heart needs 0.9ml/min/g but if the heart has to work hard this may increase four fold.
- The heart is also extremely intolerant of inadequate flow.
- Minimum: 300ml/min
- Maximum: 1200ml/min
Describe the blood flow to the kidney
- Requires high constant flow to maintain its function (3.5ml/min/g) though most flow is not nutritive.
- Minimum: 1200ml/min
- Maximum: 1200ml/min
Describe the blood flow to the Gut and Liver
- They are connected in series via the hepatic portal system
- At rest they receive 1ml/min/g
- Digestion of meal generates a substantial increase in flow.
- Short term flow reduction is tolerable.
- Minimum: 1400ml/min
- Maximum: 2400ml/min
Describe the blood flow to the skin
- Skin is not metabolically very active and may be upported by 0.01ml/mi/g, though flow may increase to 1.5-2ml/min/g for thermoregulation
- Minimum: 200ml/min
- Maximum: 2500ml/min
Describe the blood flow to the rest of the body
- A fairly constant demand: 200m/min
What is the total body blood flow?
- At rest: 5L/min
- In exercise: 25L/min
- CVS must deliver the above and maintain a blood flow of 750ml/min to the brain at all times.
- It must also maintain a blood flow to heart and kidneys at al times.
- Blood flow to skeletal muscle can be very high during exercise and gut blood flow is high after a meal
How do you regulate Blood flow (so that cardiac output of the pump is distributed appropriately)?
- add resistance to the system so that blood doesn’t only flow to the parts that are the easiest to perfuse (brain is harder to perfuse due to gravity)
- Reduce the ease with which some regions are perfused in order to direct blood flow to the more difficult to perfuse regions
- Arterioles and pre-capillary sphincters are the resistance vessels.
Explan the direction of the blood
- Heart pumps blood –> arteries supply –>. arterioles supply –> capillaries drain into –> venules drain into –> veins return blood –> heart
- Heart is two pumps in series. The left heart pumps blood around the systemic circulation. The right heart pumps blood around the pulmonary circulation.
The total flow in the system has to be able to change. What does this require?
- A temporary store of blood which can be returned to the heart at a different rate.
- Veins have thin walls which can easily distend or collapse enabling them to act as a variable reservoir for blood.
- The reservoir can then be called up to cope with temporary imbalances between the amount of blood returning to the heart and the amount that it is required to pump out.
- This store is in the veins.
Explain the distributon of blood in the CVS
- 67% veins
- 11% arteries anD arterioles
- 5% capillaries
- 17% heart and lungs
Where is blood flow fastest?
- Where the total cross sectional area is least:
- Cross sectnal area of aorta = 2.5cm(2) so fast flow (as the arteries branch, the total cross sectional area of the vascular bed increases)
- Total cross setional area of capillries = 4500cm(2) so slow flow)
- Combined cross-sectioal area of vena cavae = 8cm(2) so slightly faster flow
Describe the great arteries arising from the heart
- Carry blood flow away from the heart to the capillary beds
- Pulmonary trunk arisng fom the right ventricle. It bifurcates into the right and left pulmonary arteries that enter the lungs
- Aorta is the major artery arising from the left ventricle. It courses in a posteriorly oblique arch to descend into the thoracic cavity.
- 3 main arterial trunks: the brachiocephalic artery, the left common carotid artery and the left subclavian artery arise from the arch of the aorta. They are elastic arteries
What are the 3 Major Types of Arteries?
- Elastic conducting arteries (widest diameter)
- Muscular distributing arteries (intermediate diameter)
- Arterioles (narrowest)
Describe Elastic Arteries
- Systole: LV contraction causes the blood pressure n the aorta to rise to ~120mHg. The walls of the elastic aorta and other elastic arteries stretch.
- Diastol: aorti semilunar valve closes. Walls of aorta recoil maintaining pressure on the blood and moving it towards the smaller vessel. Aortic pressure drops to 70-80mmHg (diastolic)
- So elastic arteries conduct blood away from the heart but also act as pressure reservoirs. During diastole they act as auxiliary pumps giving back the elastic energy stored during systole.
Describe the Characteristics of Elastic Arteries
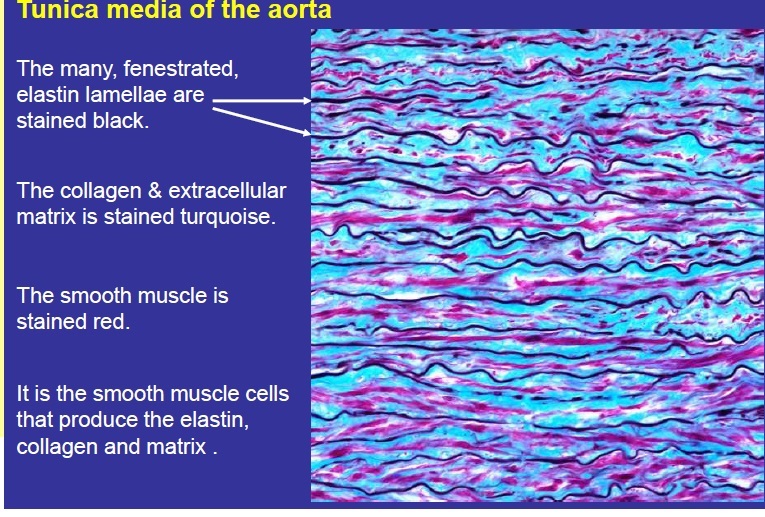
- Tunica intima: endothelial cells with long axis orientated parallel to the long axis of artery. Narrow subendothelium of connective tissue with discontinuous internal elastic lamina
- Tunica media: 40-70 fenestrated (contains holes) elasticmembranes. Smooth muscle cells (producing collagen , elastin and extracellular matrix) between these lamellae. Thin external elastic lamina may be present. Branching elastic lamellae.
- Tunica adventitia: thin layer of fibroelastic connective tissue (contains collagen), vasa vasorum (‘vessels of vessels’), lymphatic vesels and nerve fibres (has got neurovascular supply)