Describe the relationship between the systemic and pulmonary circulations.
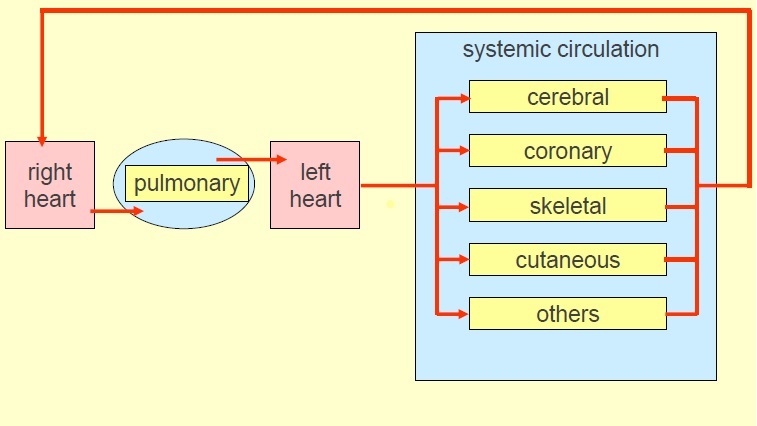
The entire output of the right heart is directed through the pulmonary circulation which is supply driven - it must accommodate the entire cardiac output, whatever the systemic circulation determines it to be.
The systemic circulation is demand led.
Pulmonary circulation is in series with all the systemic circulations.
Systemic circulations are in parallel to each other.
Describe the dual circulation of the lungs
Bronchial circulation is part of the systemic circulation and meets metabolic requirements of most parts of the lungs (parts of the lungs that are not well-perfused by the pulmonary circulation e.g. the bronchi and bronchioles).
Pulmonary circulation: blood supply to alveoli – required for gas exchange
Describe the 2 main features of the pulmonary circulation
Low resistance due to:
Short wide vessels
Lots of capillaries (high density, high capillary surface area, connected together in parallel)
Arterioles have relatively little smooth muscle.
The pulmonary circulation works with low pressure and low resistance.
If the pressure is too high, this could lead to pulmonary oedema and rupture of fine capillaries.
State the normal pressures in the pulmonary artery, pulmonary capillaries and pulmonary veins
Pulmonary artery: mean pressure: (~12-15mmHg; changes in arterial pressure can have an effect on capillary pressure due to the low resistance)
Pulmonary capillary: mean pressure: (~9-12 mmHg; lower than in systemic circulation).
Pulmonary vein: mean pressure: (~2-5mmHg)
What are the adaptation of the pulmonary circulation to promote efficient gas exchange?
Large capillary surface area due to very high density of capillaries in alveolar wall.
Short diffusion distance due to very thin layer of tissue separating gas phase from plasma; combined endothelium and epithelium thickness is ~0.3 micrometres
Large surface area and short diffusion distance produce high O2 and CO2 transport capacity.
Movement of molecule is always down a concentration gradient.
Explain the concept of ventilation perfusion matching in the pulmonary circulation
For efficient oxygenation, the ventilation of alveoli needs to match perfusion of alveoli.
The optimal ventilation/perfusion ratio = 0.8
If there is a ventilation/perfusion mismatch, the blood leaving the lungs will contain less oxygen and hypoxia will result.
Maintaining this ratio means diverting blood from alveoli which are not well ventilated (e.g. Due to disease or mucus plug) as the blood leaving these alveoli is not well oxygenated.
What is the so-called physiological shunt?
Many cardiovascular and respiratory conditions lead to ventilation/perfusion mismatch and even in normal lungs there is a small mismatch because of the way in which gravity increases blood flow to the base of the lungs when more air is delivered to the apices.
This leads to some blood passing through the lungs without being properly oxygenated - the so-called physiological shunt.
Why is tissue fluid formation not normally formed in the lungs?
The pressure in the pulmonary capillaries is normally less than the colloid osmotic pressure.
What is the main mechanism that ensures optimal ventilation perfusion ratio?
There is no overall control of the pulmonary resistance but the pulmonary arterioles can control the distribution of the cardiac output to the lung.
Blood is generally directed away from areas where oxygen uptake is reduced by hypoxic pulmonary vasoconstriction.
Hypoxic pulmonary vasoconstriction is the most important mechanism in regulating pulmonary vascular tone.
Alveolar hypoxia results in vasoconstriction of pulmonary vessels, and the increased resistance means less flow to poorly ventilated areas and greater flow to well ventilated areas.
This mechanism ensures that perfusion matches ventilation. Poorly ventilated alveoli are less well perfused.
Helps to optimise gas exchange.
What can chronic hypoxic vasoconstriction lead to?
Chronic hypoxia can occur at altitude or as a consequence of lung disease such as emphysema.
Chronic increase in vascular resistance due to chronic vasoconstriction leads to chronic pulmonary hypertension.
High afterload (too much pressure) on right ventricle (as it has to pump against high resistance) can lead to right ventricular heart failure.
Describe how gravity influences low pressure pulmonary vessels
Gravity creates hydrostatic pressure in a column of blood (or any fluid) which therefore allows posture to influence the distribution of fluid flow through the lungs.
When standing upright, transmural pressure within the blood vessels at the base of the lungs is elevated by the increase in hydrostatic pressure.
This may lead to some filtration of tissue but will also distend the vessels and increase flow to those areas.
In the upright position (orthostasis), there is greater hydrostatic pressure on vessels in the lower part of the lung.
Above the heart, the vessels collapse during diastole.
At the same level as the heart, the vessels are continously patent.
At a lower level to the heart, the vessels are distended (due to the hydrostatic pressure). It is more difficult to maintain the ventilation perfusion ratio.
What is the effect of exercise on pulmonary blood flow?
Increased cardiac output
Small increase in pulmonary artery pressure
Opens apical capillaries
Increased O2 uptake by lungs
As blood flow increases capillary transit time is reduced
At rest transit time is ~1s. Can fall to ~0.3s without compromising gas exchange because gas exchange is so efficient.
Describe the forces which are involved in the movement of fluid
Starling forces determine tissue fluid formation.
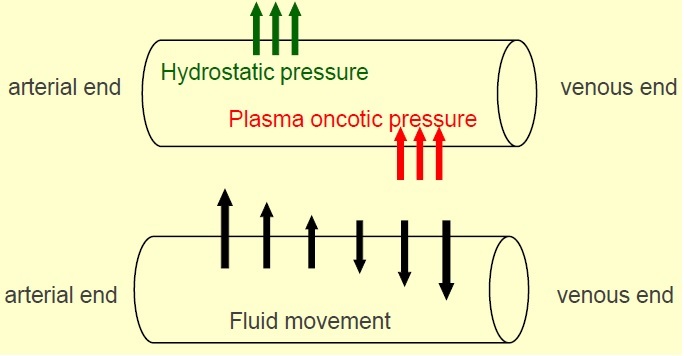
Hydrostatic pressure of blood within the capillary pushes fluid out of the capillary.
Oncotic pressure (colloid osmotic pressure) within the capillary is the pressure exerted by large molecules such as plasma proteins, draws fluid back into the capillary.
Capillary hydrostatic pressure is influenced more by venous pressure in the systemic circulation; fluid moves out at arterial end (higher hydrostatic pressure) and in at venous end (lower hydrostatic pressure).
Balance between hydrostatic and plasma oncotic pressure determines amount of fluid that moves out.
Venous pressure has the greatest effect in capillary hydrostatic pressure so in the low pressure pulmonary system, what happens?
Low capillary pressure minimises the formation of lung lymph - only a small amount of fluid leaves the capillaries.
Filtration approximately equals reabsorption (Some tissue fluid is formed but the lungs can cope with this without fluid build up.)
Increased capillary pressure causes more fluid to filter out (filtration > reabsorption) –> Oedema (which is normally prevented by low capillary pressure).
Increased venous pressure –> increased hydrostatic pressure.
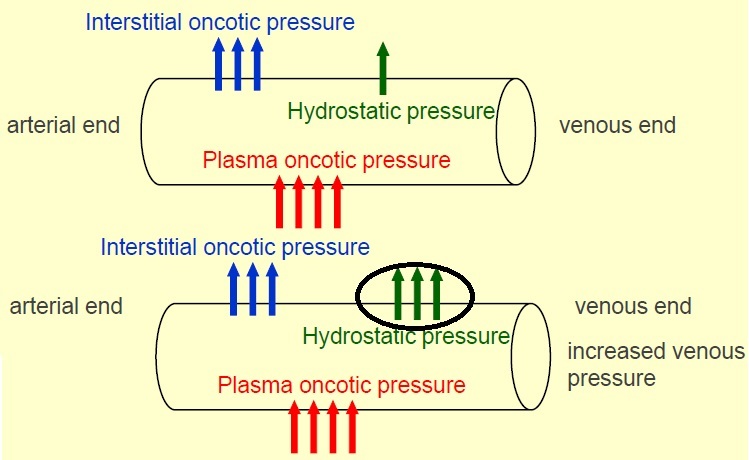
Why might capillary pressure increase?
If the left atrial pressure rises to 20-25mmHg e.g. Due mitral valve stenosis or left ventricular failure.
What is the effect of Pulmonary Oedema?
Impairs gas exchange.
Affected by posture (changes in hydrostatic pressure due to gravity).
The fluid is mainly at the base of the lungs when upright
redistribution occurs when lying down - increased hydrostatic pressure at the top of the lungs –> increased pulmonary oedema throughout the lung,
Use diuretics to relieve symptoms.
Treat underlying cause.
Describe the O2 demand of the cerebral circulation
The brain has a high O2 demand - needs constant supply of O2.
Receives 15% of cardiac output but only accounts for 2% of body mass.
O2 consumption of grey matter accounts for ~20% of total body consumption at rest.
Must produce a secure O2 supply (neurones cannot last long without a supply of oxygen).
How is the Cerebral Circulation able to meet the high demand for O2?
High capillary density with a large surface area for gas exchange and reduced diffusion distance (<10 micrometres between neurone and capillary).
High basal rate flow - 10x faster than body average
High O2 extraction - 35% above average.
Why is a secure O2 supply to the brain vital?
Neurones are very sensitive to hypoxia.
Loss of consciousness after a few seconds of cerebral ischaemia.
Begin to get irreversible damage to neurones in ~4 minutes.
An interruption to the blood supply e.g. A stroke, causes neuronal death.
How is a secure cerebral blood supply ensured?
Structurally
Functionally
How is a secure cerebral blood supply ensured structurally?
Anastomoses between basilar and internal carotid arteries - ‘Circle of Willis’: if one part of the circle becomes blocked or narrowed (stenosis) or one of the arteries supplying the circle is blocked or narrowed, blood flow from the other blood vessels can often preserve the cerebral perfusion well enough to avoid the symptoms of ischaemia.
How is a secure cerebral blood supply ensured functionally?
Brainstem regulates other circulations.
Myogenic Autoregulation maintains perfusion during hypotension
Metabolic factors control blood supply.
How does Myogenic Autoregulation help ensure secure blood supply to the brain?
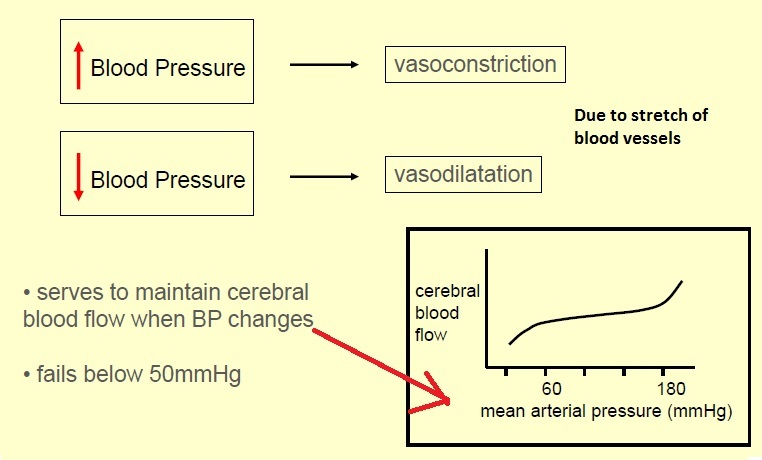
Cerebral resistance vessels have a well developed Myogenic response to changes in transmural pressure (pressure across the wall).
Increased blood pressure –> vasoconstriction
Decreased blood pressure –> vasodilatation.
This serves to maintain cerebral blood flow when BP changes
Fails below 50mmHg
How do Metabolic Factors help ensure secure blood supply to the brain?
Metabolic regulation: cerebral vessels are very sensitive to changes in pCO2 (partial pressure).
Metabolic factors control blood flow.
Hypercapnia: increased pCO2 –> vasodilatation
Hypocapnia: decreased pCO2 –> vasoconstriction.
Panic hyperventilation (blowing off lots of CO2) can cause hypocapnia and cerebral vasoconstriction leading to dizziness or fainting (loss of consciousness - syncope).
As soon as this happens, panic hyperventilation resolves itself.




