Does the Sodium Pump set the Resting Membrane Potential?
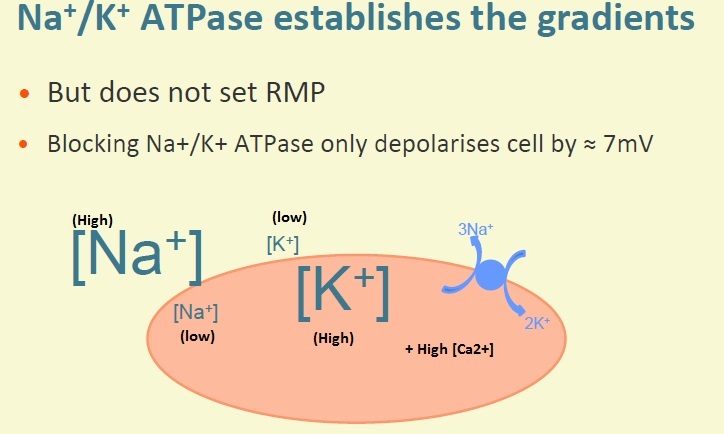
The Na+/K+-ATPase establishes the ionic gradients but does not set the resting membrane potential
Blocking the Na+/K+-ATPase only depolarises cell by approximately ~7mV.
What sets the Resting Membrane Potential?
RMP is set largely due to K+ permeability of the cell membrane at rest. K+ channels (background inward rectifier type) are open at rest (high intracellular [K+] and low extracellular [K+]) so K+ ions move out of the cell down their concentration gradient.
The small movement of positively charged ions out of the cell makes the inside more negative with respect to the outside. As charge builds up, an electrical gradient is set up.
Resting membrane potential moves towards E(K)
Why doesn’t RMP = E(K)
Very small permeability to other ion species at rest (other electrochemical gradients present)
What effect do action potentials have on cardiac myocytes?
APs trigger increase in cytosolic [Ca2+]
A rise in calcium is required to allow actin and myosin interaction - generated tension
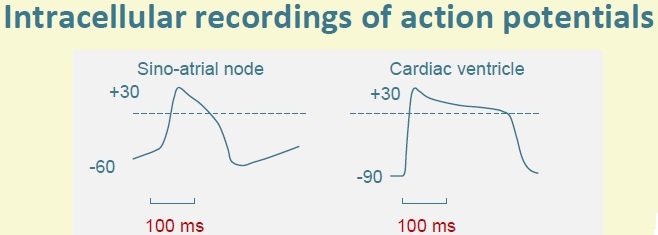
Draw the changes in membrane potential of cardiac ventricular and sinoatrial node pacemaker cells, including time durations
Describe the membrane permeability changes and ionic currents underlying the ventricular (cardiac) action potential
Opening voltage-gated fast Na+ channels causes a large rapid upstroke leading to a Na+ influx which drives membrane potential to E(Na)
But E(Na) is not reached because of Na+ channel rapid inactivation and because of the permeability for other ions.
Initial depolarisation occurs - transient outward K+ current is caused by a specific type of K+ channels which open briefly before closing (voltage gated i(to)). The plateau region is caused by the opening of voltage-gated Ca2+ (L type) channels (some K+ channels also open).
The influx of [Ca2+] drives the membrane potential to E(Ca) (~+120mV) BUT this is not reached because of other open channels (K+). So the plateau region stays around 0mV - balanced with K+ efflux.
The downward stroke (repolarisation) is caused by the inactivation of Ca2+ channels (which take much longer to inactivate than Na+ channels) and the opening of voltage-gated K+ channels which allow an efflux of K+ and other K+ channels.
What happens when the heart muscle is relaxed?
During diastole, the potential difference between inside and outside of the cells is negative inside. Except for the pacemaker cells, this potential difference is constant during diastole.
Describe the cardiac action potential duration
About 280ms at rest because of the plateau sustained mainly by calcium channels.
Length of the AP is crucial; once the AP has begun in any part of the heart it needs to be long enough for the cell still to be depolarised when the last cell of the myocardium starts its zap. Therefore one AP in the pacemaker generates just one AP in every cell of the heart. This will produce a single heart beat.
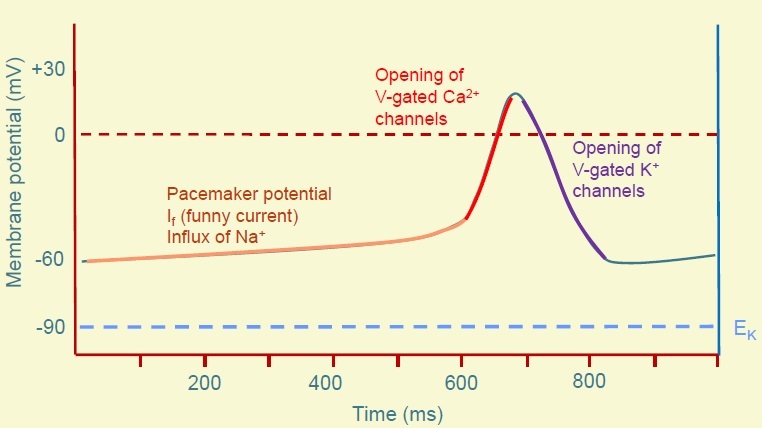
What is the Pacemaker Potential?
No stable resting membrane potential - just a long slow period of depolarisation (the diastolic period) which is called the pacemaker potential.
The pacemaker potential is the initial slow to threshold (I(f) funny current). It is activated by membrane potentials more negative than -50mV. The more negative the membrane potential, the more HCN channels are activated.
What are HCN channels?
Hyperpolarization-activated Cyclic Nucleotide-gated Channels
Activated by Hyperpolarization
Activated by binding some molecules such as cAMP
Allows influx of Na+ channels Responsible for the pacemaker potential - the long period of slow depolarisation during diastole in SA node cells.
Describe the SA Node action potential
After the pacemaker potential, the upstroke is caused by the opening of voltage-gated Ca2+ channels (fast Na+ channels are all in an inactive state due to the persistently less negative membrane voltage)
The downward stroke is (repolarisation) caused by the opening of voltage-gated K+ channels (K+ efflux) and closure of the Ca2+ channels.
The HCN channels open during the repolarisation of the cell as the potential approaches its most negative values.
Describe Action Potentials throughout the heart
Action potential varies throughout the heartheart.
The sinoatrial node is fastest to depolarise so it sets the rhythm (is the pacemaker) but OTHER PARTS OF THE CONDUCTING SYSTEM (e.g.purkinje fibres, AV node) also have automaticity but they are slower.
Describe the characteristics of cardiac myocytes
Single central nucleus
Cells joined together at intercalated discs
Gap junctions found on intercalated discs (large ion channels formed by connexon proteins) are NON-SELECTIVE - permeable to a wide range of ions. Gap junctions permit movement of ions and electrically couple cells (movement of positively charged ions pout of cell causes depolarisation)
Desmosomes are also found on intercalated disks - RIVET cells together. Cells are mechanically tethered together to contract together.
Describe how the intracellular [Ca2+] increases
Depolarisation opens L-type Ca2+ channels in T Tubule system
Localised Ca2+ entry (via the L-type channels) opens Calcium-Induced Calcium Release (CICR) channels in the sarcoplasmic reticulum.
Close link between the L-type channels and Ca2+ release channels. 25% of intracellular [Ca2+] enters across sarcolemma (L-type channels) and 75% of intracellular [Ca2+] is released from SR, causing the intracellular [Ca2+] to rise during the plateau phase.
Release of Ca2+ can’t take place until Ca2+ enters across sarcolemma first. Ca2+ binds to TnC subunit causing a conformational shift so Tropomyosin moves away and unblocked the myosin binding site on the actin filament.
What is the Sliding Filament Theory?
1) Attachment: myosin head tightly bound to actin molecule.
2) Release: ATP binds to the myosin head causing it to uncouple from the actin filament.
3) Bending: hydrolysis of the ATP caused the uncoupled myosin head to bend and advance a short distance (5nm)
4) Force Generation: the myosin head binds weakly to the actin filament causing release of inorganic phosphate which strengthens binding and causes the power stroke in which the myosin head returns to its former position.
5) Reattachment: ATP binds to the myosin head causing detachment from actin. The cycle will repeat.
Individual myosin heads attach and flex at different times causing movement. Muscle shortens as the thick and thin filaments slide past each other.
Describe Relaxation in Cardiac Myocytes
Intracellular [Ca2+] must return to resting levels in order for relaxation to take place.
Most is pumped back into the SR by SERCA which is stimulated by raised Ca2+ levels.
Some Ca2+ exits across cell membrane via Sarcolemmal Ca2+ ATPase and Na+/Ca2+ Exchanger,
In the heart, the force generated in a cell, at a given degree of stretch is proportional to Ca2+ concentration. Therefore the force of contraction depends upon the balance between the rate of entry of Ca2+ into the cytoplasm and its rate of removal. As the plateau phase is long, the muscular contraction is sustained for 200-300ms which is essential for the normal pumping activity of the heart.
How is tone of blood vessels controlled?
Vascular smooth muscle within the tunica media is not striated.
Contraction still takes place but myofilaments are arranged differently.
Gap junctions are still present (aqueous pores allowing ion movement) and they electrically couple cells.
Contraction of these vascular smooth muscles leads to an increased tone of the vessel, narrowing the lumen.
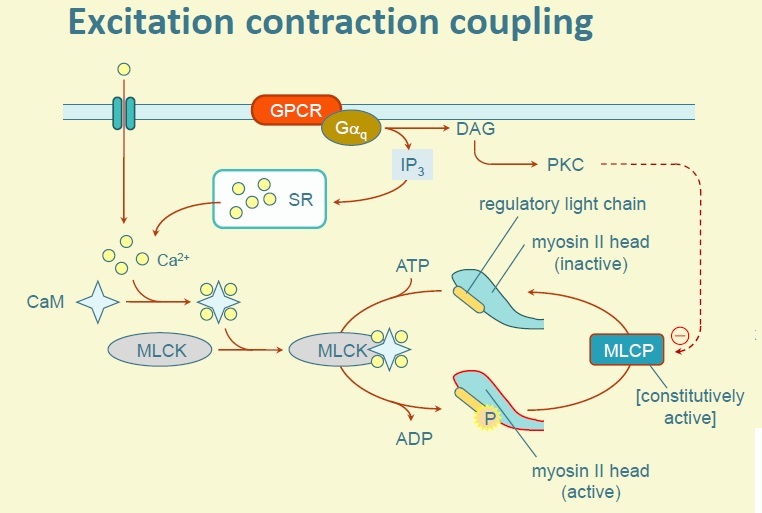
How does binding of Ca2+ to Calmodulin control excitation coupling?
Binding of Ca2+ to Calmodulin activates Myosin Light Chain Kinase (MLCK) which phosphorylates the myosin light chain to permit interaction with actin.
Myosin Light Chain must be activated (via phosphorylation by MLCK) to enable actin-myosin interaction which in turn leads to contraction.
Relaxation occurs as Ca2+ levels decline.
Phosphorylating by Protein Kinase A inhibits MLCK therefore inhibiting contraction.
Why is the Pacemaker Action Potential different to the Cardiac Action Potential?
Pacemakers initiate the AP themselves rather than by conduction of excitation from surrounding cells. In diastole, the membrane potential is unstable - depolarises steadily (pacemaker potential).
This is thought to be due to the HCN channels that are permeable to Na+ ions which are different to the fast Na+ channels - they are activated by Hyperpolarization, referred to as the funny current. Pacemaker cells do not have fast Na+ channels but as the membrane depolarises with the pacemaker potential, voltage gated Ca2+ channels eventually open producing a faster rate of depolarisation to a positive membrane potential.
The opening of these Ca2+ channels is not sustained - there is no plateau and the action potential is triangular in shape.
As soon as the membrane is repolarised back to -600mV, it begins to depolarise again slowly - the next pacemaker potential begins until threshold is reached again and the next AP occurs.
Describe the Action Potential in the Conducting Fibres
Purkinje fibres conduct excitation through the ventricular myocardium.
They have long APs but within the AV node and the bundle of His, there are cells capable of pacemaker activity.
Their natural rate is much slower than the SA node so they are normally overridden.
If however there is a conduction block, they may become important.
The ANS is an efferent system. It is important for regulation many physiological functions - what physiological functions?
Heart rate,
blood pressure,
body temperature etc (homeostasis - keeping everything in balance)
Coordinating the body’s response to exercise and stress
Largely outside voluntary control
Give examples of what the ANS exerts control over
Smooth muscle (vascular and visceral)
Exocrine secretion e.g. Saliva and sweat
Rate and force of contraction in the heart
Describe the divisions of the ANS
Based on anatomical grounds: Parasympathetic nervous system Sympathetic nervous system
NB: some textbooks include a third division: the enteric nervous system (network of neurones surrounding GI tract is normally controlled via sympathetic and parasympathetic fibres)
Describe the organisation of sympathetic and parasympathetic systems (generally)
Two neurones arranged in series
Cell body of Preganglionic neurone in the CNS
Other neurone is located entirely outside of the CNS
Cell bodies of these neurones are located in structures knwon as ganglia
Preganglionic fibres leave the CNS and then synapse with post-ganglionic cell bodies in the ganglia.
Post-ganglionic fibres run to the innervated structures and form neuro effect junctions with effector cells
Transmission at both ganglionic synapses and neuro effector junctions is by the release of chemical messengers - neurotransmitters.

