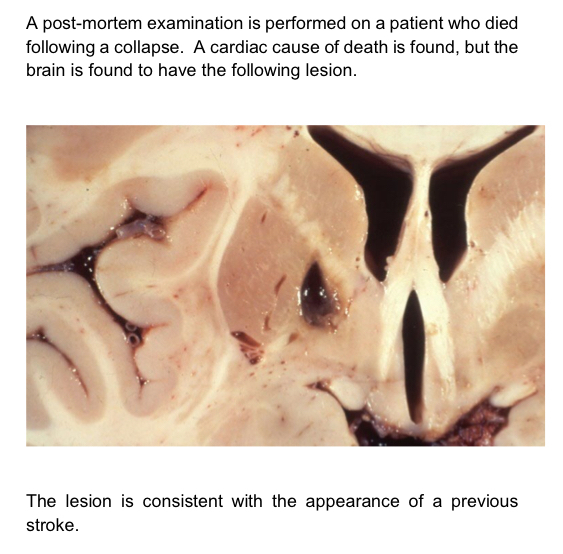
What is the definition of a stroke and a TIA?
- Stroke: a ‘cerebrovascular accident’, is a ‘serious life threatening condition that occurs when the blood supply to part of the brain is cut off’. The symptoms and signs persist for more than 24 hours and cause an infarction
- TIA: have similar clinical features of a stroke but completely resolve within 24 hours as only temporary blockage

What are the different categories of strokes?
- Ischaemic (85%): thromboembolic
- Haemorraghic (10%): subarachnoid, intracerebral
- Other (5%): dissection, venous sinus thrombosis (occlusion of veins causes backpressure and ischaemia due to reduced blood flow), hypoxic brain injury (e.g after MI)
Why shouldn’t you give aspirin when you suspect a stroke?
Need to wait till youve done a CT to see if haemorraghic as if so could make things worse
How do we manage strokes in the ED?
- Are they within the window for thrombolysis (<4 hours)?
- Do a CT head to determine if it is a bleed (if bleed cannot
proceed with thrombolysis)
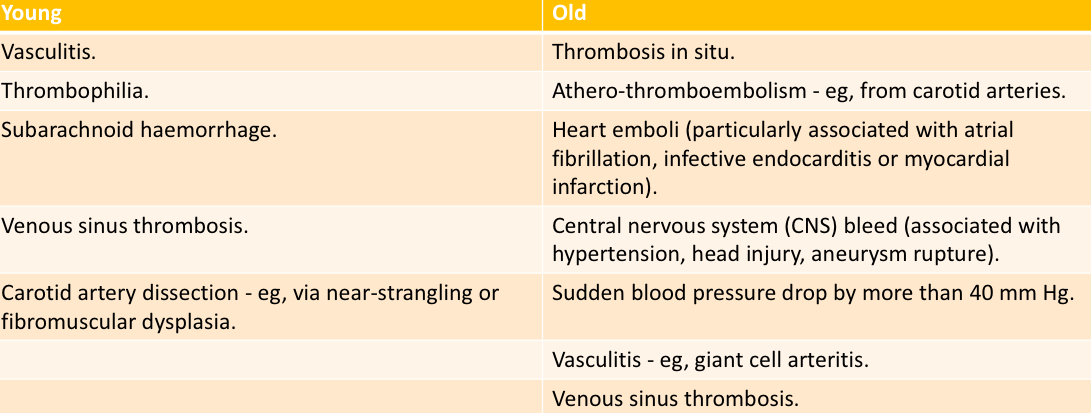
What are some risk factors for a stroke?
- AF, Endocarditis and Valvular disease can all form clots
- Bifurcation of carotids atherosclerosis

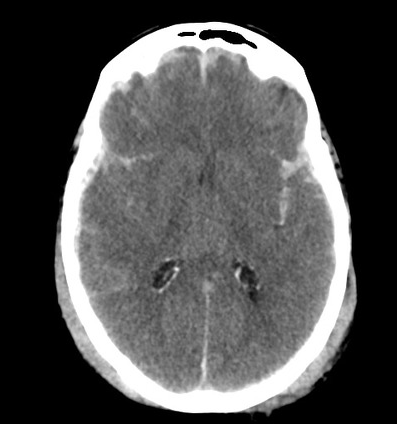
What does a stroke look like on imaging?
CT: bleed will show up as bright white with possible mass effect, ischaemia won’t show up early on but as it establishes it becomes hypodense
MRI: rarely done due to takes a long time, ischaemia shows up as high energy signal

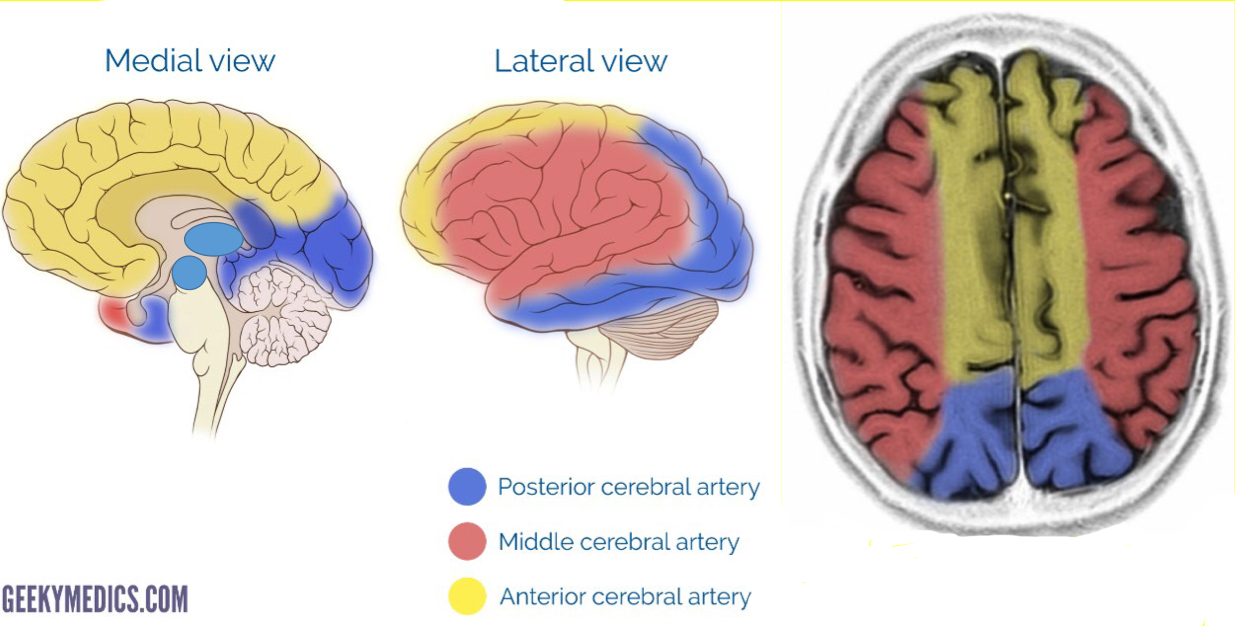
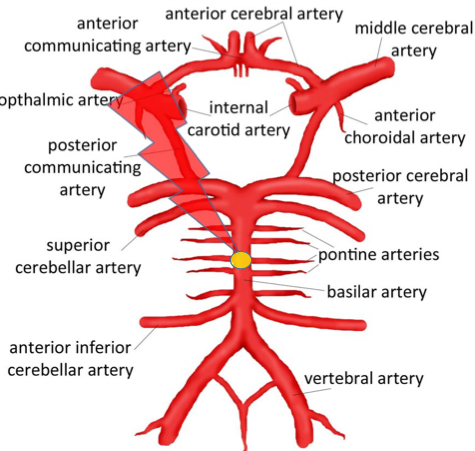
Describe the general blood supply to each lobe of the brain?
ACA: medial
MCA: lateral
PCA: also supplies midbrain and thalamus
What stroke syndrome would you get if somebody had a stroke involving the anterior cerebral artery?
- Contralateral lower limb and genital weakness
- Contralateral lower limb and genital sensory deficit
- Urinary incontinence (paracentral lobule that has excitatory and inhibitory neurones on M centre is damaged)
- Split brain or Alien Hand Syndrome (corpus callosum)
- Apraxia (left frontal lobe, cannot motor plan)
- Posible dysarthria/aphasia
- Frontal lobe features (e.g sexual disinhibition, personality changes)

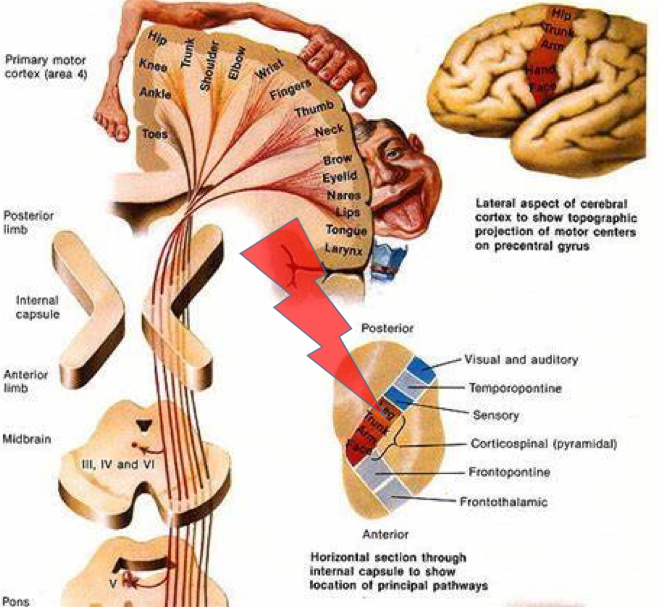
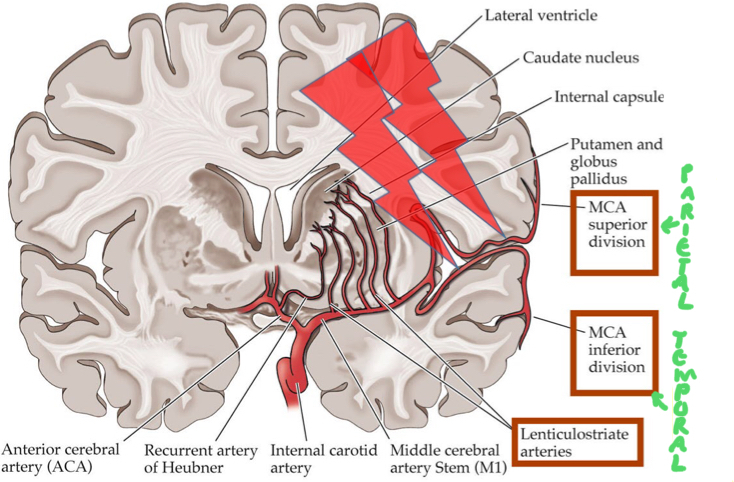
What stroke syndrome would you get if somebody had a stroke involving the proximal middle cerebral artery?
- Contralateral full hemiparesis (face, arm and leg affected as internal capsule affected)
- Contralateral sensory loss (mainly face and arm due to homunculus but larger areas if internal capsule involved)
- Contralateral homonymous hemianopia without macular sparing (both optic radiations wiped out)
- Global aphasia (if left hemisphere affected)
- Contralateral neglect (if lesion in right parietal lobe)
Why does a stroke occuring in the MCA have such a high mortality rate?
- Widespread and can cause cerebral oedema
- Can turn haemorraghic if vessels in infarcted area break down
What is hemispatial neglect?

- Mainly left neglect when right parietal lobe damaged
- Not acknowledging the left side of space or even your own body exists. Visual fields normal
- Tactile extinction
- Visual extinction
- Anosognosia (won’t acknowledge theyve had a stroke)

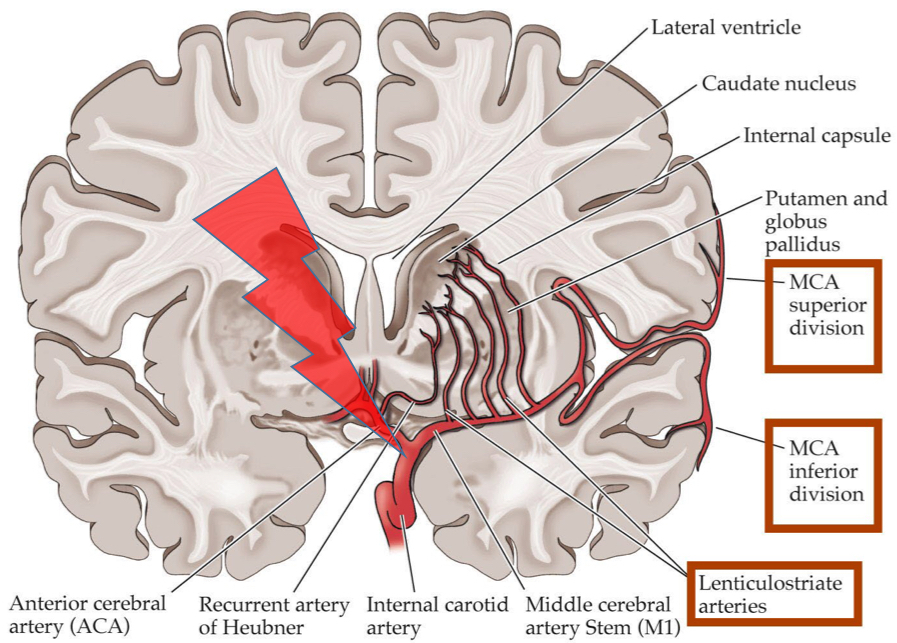
What stroke syndrome would you get if somebody had a stroke involving the lenticulostriate arteries?
Lacunar strokes: Destruction of small areas of internal capsule and basal ganglia
- Can distinguish from MCA strokes as no cortical features like neglect and aphasia
- Pure motor, pure sensory (thalamoperforator arteries supplying thalamus), sensorimotor
- Contralateral effects as in internal capsule
What stroke syndrome would you get if somebody had a stroke involving the distal middle cerebral artery?
Superior division:
- Lateral frontal lobe
- Contralateral face and arm weakness due to motor cortex
- Expressie aphasia as Broca’s area affected if left sided
Inferior division:
- Lateral parietal and temporal lobe
- Contralateral sensory loss in face and arm due to sensory cortex
- Receptive aphasia as Wernicke’s area affected if left sided
- Contralateral homonymous hemianopia with no macular sparing (both optic radiations)
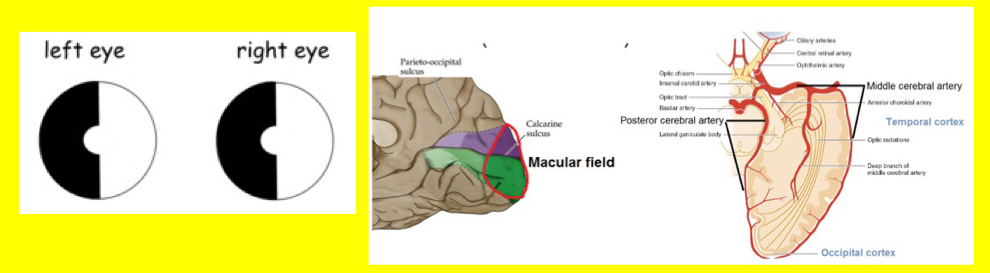
What stroke syndrome would you get if somebody had a stroke involving the posterior cerebral artery?
- Contralateral homonymous hemianopia (with macular sparing due to collateral supply from MCA)
- Contralateral sensory loss due to damage to thalamus
What stroke syndrome would you get if somebody had a stroke involving the cerebellum?
- N+V, vertigo, headache, dizziness
- DANISH signs ipsilateral
- Possible ipsilateral brainstem signs since cerebellar arteries
supply brainstem as they loop round to the cerebellum
- Possible ipsilateral Horner’s syndrome (sympathetics travel lateral brain stem with cerebellar arteires)
- Possible contralateral sensory signs as predecussation

How do brainstem strokes present?
- Contralateral limb weakness with ipsilateral cranial nerve signs
- Due to damage of corticospinal tracts above decussation pyramids and damage to cranial nerve nuclei on the same side
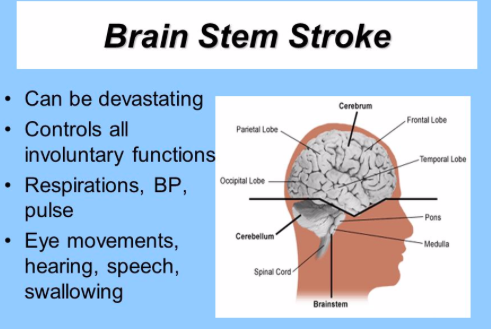
What stroke syndrome would you get if somebody had an occlusion of the distal basillar artery?
- Can cause sudden death as vessel supplies brainstem and cardiorespiratory centres
- Visual and oculomotor deficits as branches into midbrain for CNIII nuclei and joins with PCA to supply PVC in occipital
- Behavioural abnormalities
- Somnolence, hallucinations and dream like behaviour as brain stem controls sleep
- Motor function in tact as cerebral peduncles can get blood from PCA

What stroke syndrome would you get if somebody had an occlusion of the proximal basillar artery (at level of pontine branches)?
- Locked in syndrome
- Complete loss of movement of limbs
- Preserved ocular movement because midbrain is getting supply from PCAs via posterior communicating arteries
- Preserved consciousness ( because midbrain reticular formation still intact)
How do we classify stroke?
Bamford (Oxford) Stroke Classification
TACS: unilateral weakness (+/- sensory deficit) of FAL, homonymous hemianopia, higher cerebral dysfunction e.g aphasia
PACS: only 2/3 of the above
POCS: one of the following… CN palsy with contralater motor/sensory deficit, bilateral motor/sensory deficit, conjugate eye movement disorder, cerebellar dysfunction, homonymous hemianopia with macular sparing
LACS: one of the following… pure sensory deficit, pure motor deficit, sensorimotor deficit, ataxic hemiparesis

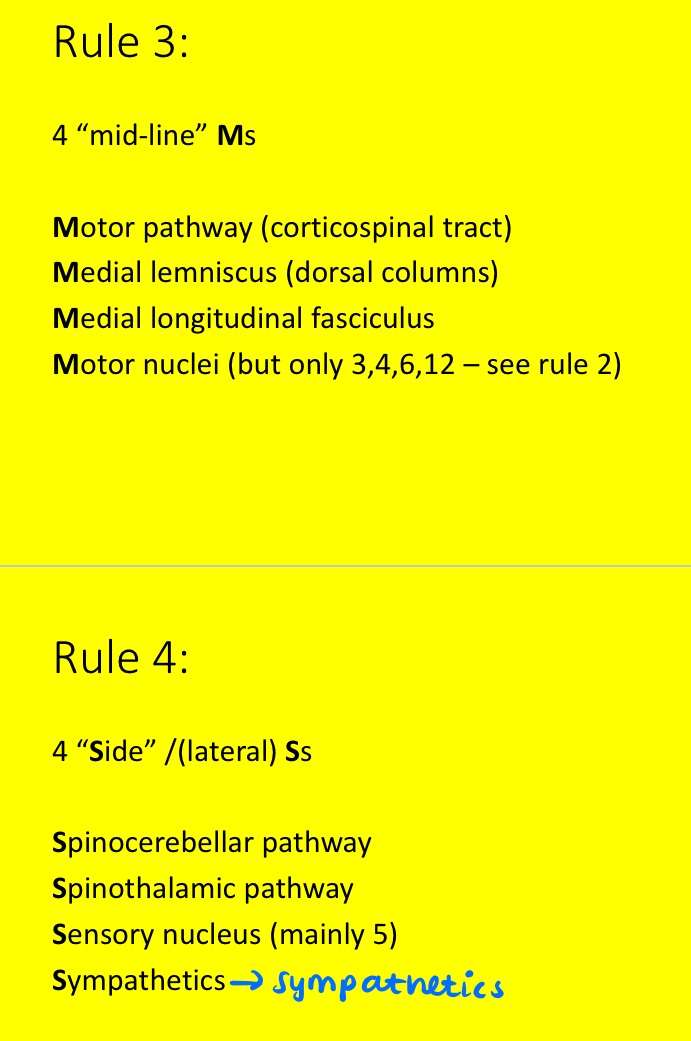
What is the rule of 4s for brainstem strokes?
- 4 CNs in each section
- 4 motor nuclei in midline and each go into 12
- 4 midline M’s
- 4 sides
Would you expect any visual field defects in this patient?
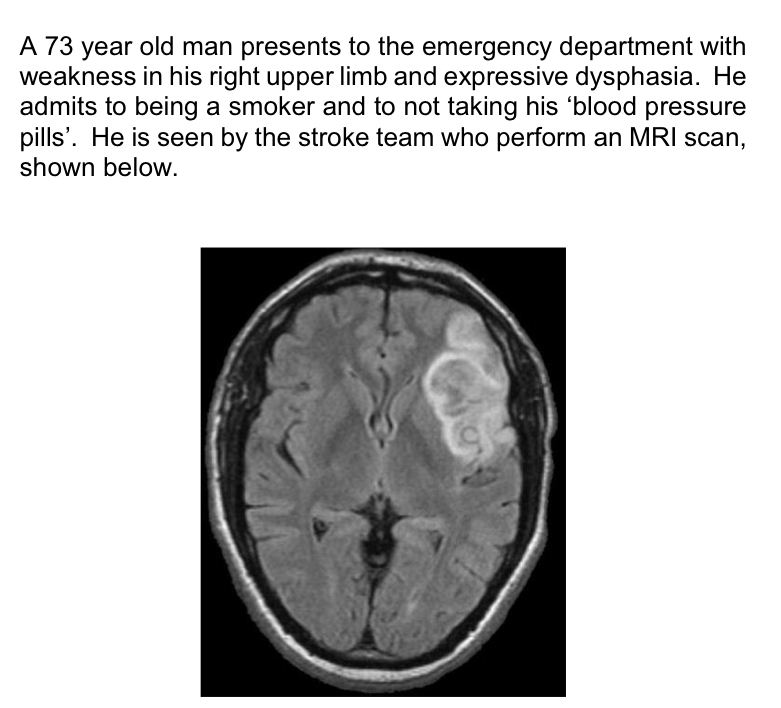
Yes - MCA occluded so will wipe out optic radiations
Which vessel is involved and why is there issues with continence?
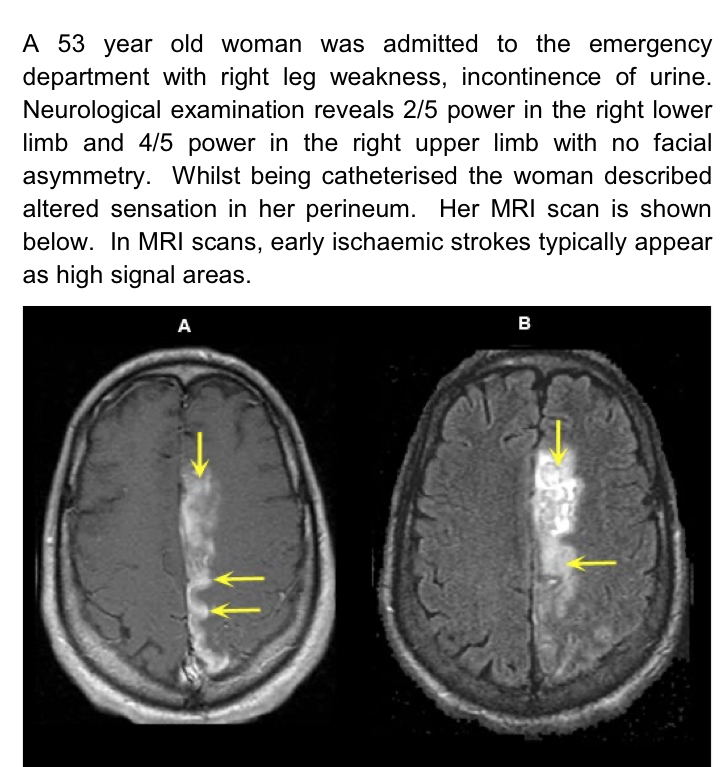
- Left ACA distal to anterior communicating artery as would be no issue if proximal to this artery as it is a circle
- Incontinence as paracentral lobule for continence is affected and genitals are near feet in sensory homunculus

Which parts of the brain have been affected and what vessel is involved?

- Occipital, thalamus and temporal
- Will have visual field defect (left homonymous hemianopia with macular sparing)
- PCA affected as supplies thalamus causing sensory issues
What Oxford classification does this belong to and how may have the patient presented?
- LACS
- Lenticulostriate arteries involved causing infarction in globus pallidus interna
- This will cause an loss of inhibition on the thalamus so excess movement contralateral to infarct






-
1 - Topography of the Nervous System30
-
2 - Embryology of the Nervous System18
-
3 - Glia36
-
4 - Somatosensory System32
-
5 - The Eye43
-
6 - Arterial Supply to the Brain17
-
7 - The Motor System40
-
8 - Movement Disorders46
-
9 - Higher Cortical Function22
-
10 - Reticular Formation and Consciousness24
-
11 - Neuropathology35
-
12 - Confusion in the Elderly36
-
13 - Headaches40
-
14 - Stroke27
-
15 - Raised ICP27
-
16 - Meningitis and Subarachnoid Haemorraghe34
-
17 - Anxiety Disorders24
-
18 - Mood Disorders28
-
19 - Psychosis31
