What are the Causes of Extraperitoneal Bladder rupture?
- Extraperitoneal, 45%
- Cause
- Pelvic fractures (bone spicule)
- avulsion tear
- Cause
- Location
* Base of bladder,
* anterolateral- Imaging
- Pear-shaped bladder
- Fluid around bladder with displaced bowel loops
- Paralytic ileus
- Imaging
- Location
- Intraperitoneal, 45%
- Cause
- Blunt trauma
- stab wounds
- invasive procedures
- Location
- Dome of bladder (weakest point)
- Imaging
- Contrast extravasation into paracolic gutters
- Urine ascites
- Cause

- Leukoplakia
- Ureteral involvement is less common than bladder and collecting system involvement.
- Leukoplakia is an uncommon lesion of the urothelium resulting from squamous metaplasia in the setting of chronic inflammation.
- Leukoplakia is characterized by plaque-like mural based filling defects which may be indistinguishable from urothelial carcinoma.
- Unlike pyeloureteritis cystica, leukoplakia is considered a premalignant lesion along the spectrum of development of squamous cell carcinoma.
- Indeed, when leukoplakia is found at one site in the urinary tract, a synchronous squamous cell carcinoma is often present.
- Malakoplakia is another cause of a plaque-like filling defect in the upper urinary tract.
- However, malakoplakia represents a granulomatous reaction to chronic inflammation and is not considered a premalignant lesion [9].
- Nevertheless, imaging differentiation of leukoplakia and malakoplakia from urothelial carcinoma is virtually impossible and tissue sampling is typically recommended.
- Treatment and prognosis
- Leukoplakia is considered a premalignant condition. There is an association with bladder neoplasia in 25% of cases.
- Differential diagnosis
- malakoplakia of the bladder
- non-neoplastic chronic granulomatous lesions due to chronic infection by Escherichia coli in an immunocompromised patient, commonly diabetes mellitus or transplant recipients
- transitional cell carcinoma
- tuberculous urethritis
- multifocal or long-segment strictures
- calcification is commonly seen
- ureteritis cystica
- reactive proliferative changes of the urothelium causing multiple small subepithelial cysts
- malakoplakia of the bladder
- https://radiopaedia.org/articles/leukoplakia-of-the-urinary-tract-1?lang=gb
- https://radiologykey.com/the-urinary-tract-renal-collecting-systems-ureters-and-urinary-bladder/
- https://pubs.rsna.org/doi/abs/10.1148/88.5.872?journalCode=radiology
What is the cause?
What isn’t this a/w
What are 3 complications?

Acquired diverticulum in bladder outlet obstruction
- Usually multiple
- Not associated with reflux
- Complications:
- Infection
- Calculi, 25%
- Tumor, 3%
Case courtesy of Dr Prat Matifoll, Radiopaedia.org, rID: 30578
What is the location of Extraperitoneal Bladder rupture?
Location
- Base of bladder
- anterolateral
What are the imaging features of Extraperitoneal Bladder rupture?
Imaging
- Pear-shaped bladder
- Fluid around bladder with displaced bowel loops
- Paralytic ileus
What are the causes of Intraperitoneal Bladder rupture?
Intraperitoneal, 45%
Cause
- Blunt trauma
- stab wounds
- invasive procedures
What is the typical location of an intraperitoneal bladder rupture?
Location
- Dome of bladder (weakest point)
What are the imaging features of an intraperitoneal bladder rupture?
Imaging
Contrast extravasation into paracolic gutters
Urine ascites
Presentation
Cerebral palsy patient with blunt abdominal trauma and haematuria.

Postvoid film shows a flame-shaped density adjacent to lateral walls of bladder representing extra-peritoneal contrast from a bladder rupture.
Case courtesy of Dr Ali Nourian, Radiopaedia.org, rID: 27806
Name the radiologic findings of extraperitoneal bladder rupture in VCUG?
A:
1- Pear-shaped bladder
2- Flame-shaped contrast extravasation into perivesical fat best seen on postvoid films
3- Paralytic ileus
https://radiopaedia.org/cases/bladder-rupture-5

Q: What is the most common type of bladder injury? hide answer
A: Extraperitoneal rupture is the most common type of bladder injury
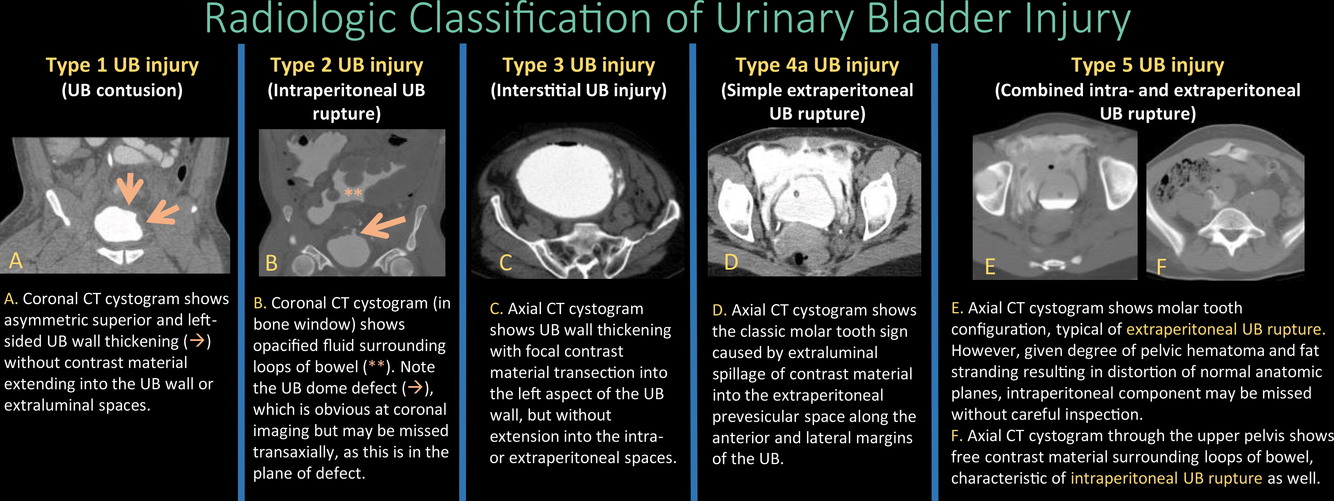
What is the classification system of bladder injury?
Classification of Bladder Injury
- Type 1: Bladder contusion
- Type 2: Intraperitoneal rupture
- Type 3: Interstitial bladder injury
- Type 4: Extraperitoneal rupture
- Type 4a: Simple extraperitoneal rupture
- Type 4b: Complex extraperitoneal rupture
- Type 5: Combined bladder injury
https://pubs.rsna.org/doi/full/10.1148/rg.2018170125
Re Bladder injury, What should preceed cystogram if there is suspicion of urethral injury?
Retrograde urethrogram
Should precede cystogram if there is suspicion of urethral injury such as blood at meatus, “high-riding” prostate, or inability to void
https://www.amboss.com/us/knowledge/Genitourinary_trauma/

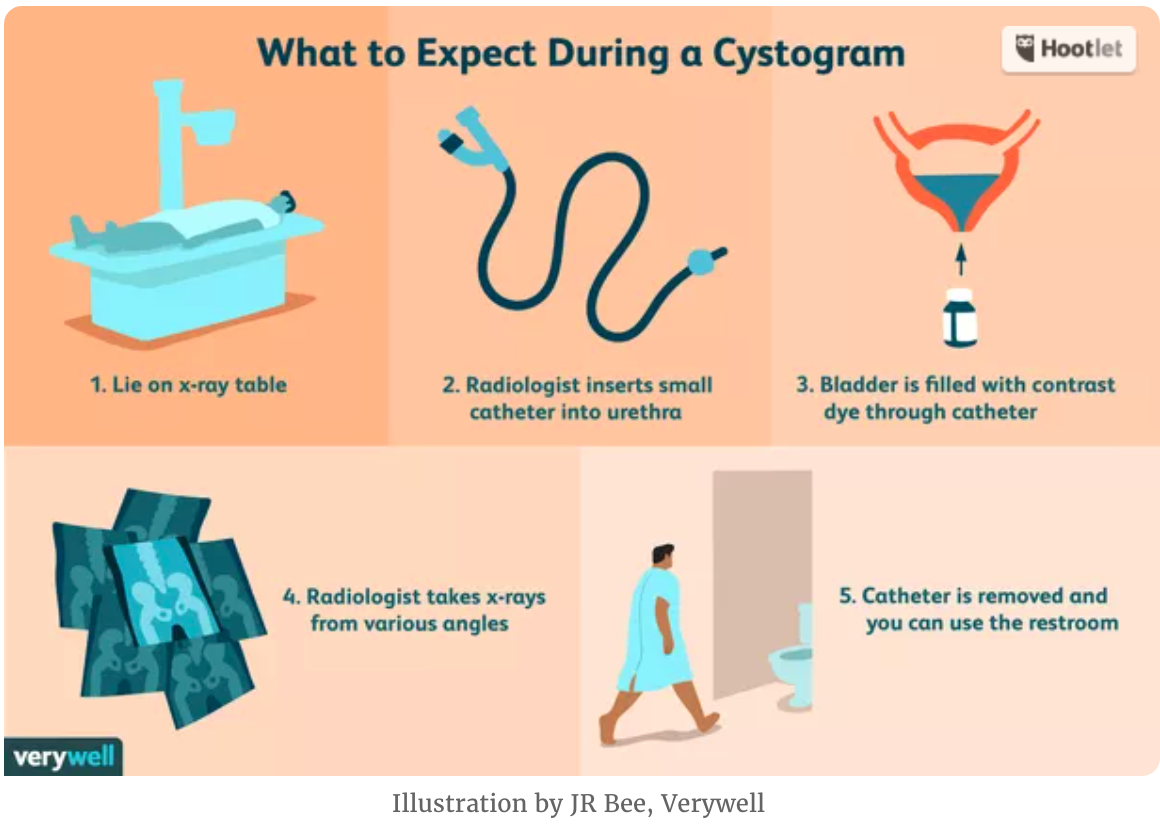
What is this procedure?
What percent of bladder ruptures are evident on post-void radiographs?

Cystogram
- Administer 350 mL of 30% water-soluble contrast
- Obtain scout view, AP, both obliques, and postvoid radiographs
- 10% of ruptures will become evident on postvoid radiographs.
https://www.verywellhealth.com/cystogram-uses-side-effects-procedure-results-4173214
What Type of examination is this?

CT cystogram
- Perform scan before the administration of intravesical contrast.
- Retrograde bladder distention is required before CT cystography.
- After Foley catheter insertion, adequate bladder distention is achieved by instilling at least 350 mL of a diluted mixture of contrast material under gravity control.
- Obtain contiguous 3–5 mm axial images from the dome of the diaphragm to the perineum, including the upper thighs.
- The normal CT cystogram will demonstrate a uniformly hyperattenuating, well-distended urinary bladder with thin walls. The adjacent fat planes will be distinct, with no evidence of extravasated contrast material.
Case courtesy of Dr Roberto Schubert, Radiopaedia.org, rID: 14924
What is this proceedure?
What is the indication?
What complication is seen here?
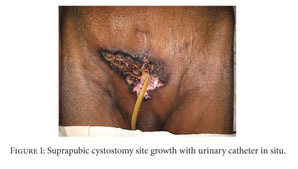
Cystostomy
Indication
• Bladder outlet obstruction
Abstract :
Patients with long-term suprapubic cystostomy can rarely develop squamous cell carcinoma (SCC) of the suprapubic cystostomy tract. In addition to the few reported cases in the literature, this paper reports a case of suprapubic cystostomy SCC in an 88-year-old man without bladder involvement. Vigilance about any abnormal lesion at the site of suprapubic cystostomy is important among health providers and patients for early detection of SCC.
https://www.google.com/url?sa=i&url=https%3A%2F%2Fgo.gale.com%2Fps%2Fi.do%3Fid%3DGALE%257CA551963159%26sid%3DgoogleScholar%26v%3D2.1%26it%3Dr%26linkaccess%3Dabs%26issn%3D2090696X%26p%3DAONE%26sw%3Dw&psig=AOvVaw3m3RiR7HgwGcuIHBBvu-7G&ust=1639441041914000&source=images&cd=vfe&ved=0CAwQjhxqFwoTCNi1oaXA3_QCFQAAAAAdAAAAABAD
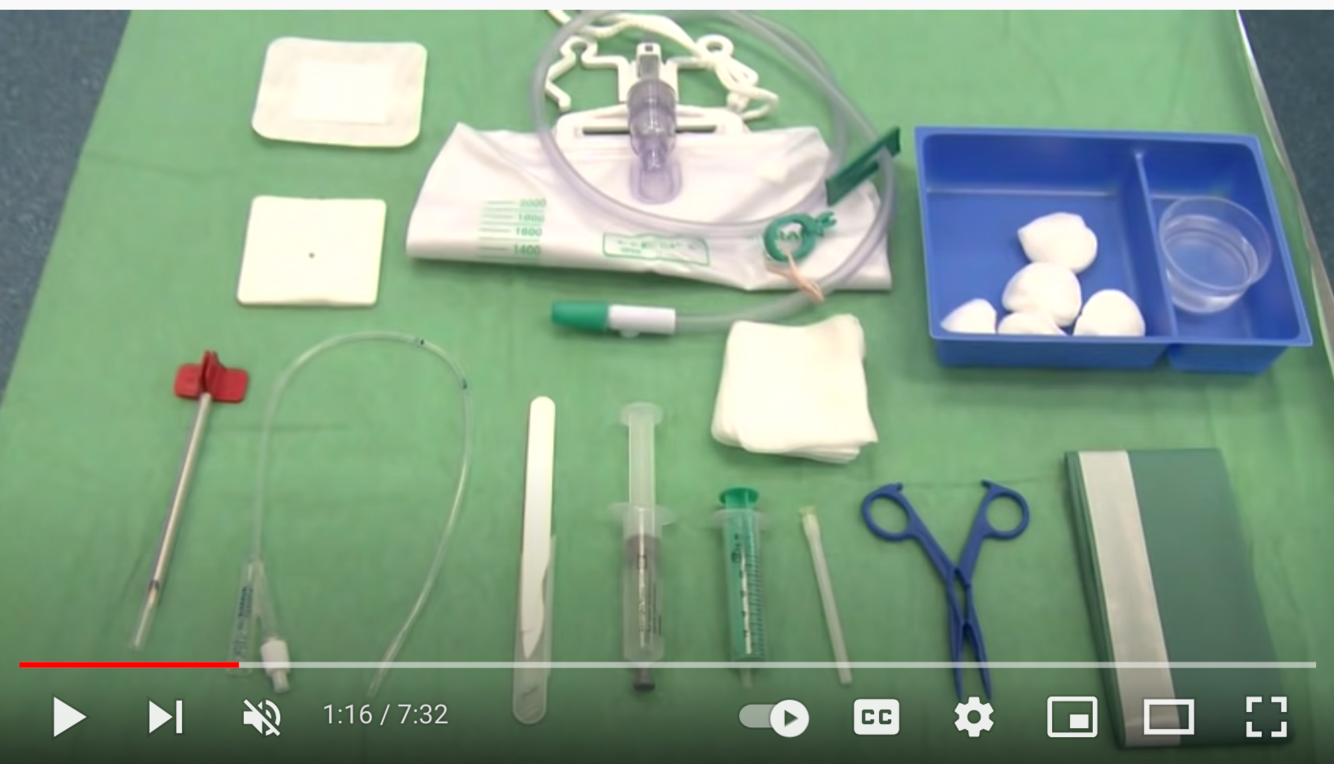
What is the proceedure for a cystostomy?
Technique
- Preprocedure workup:
- Check bleeding status
- Antibiotic coverage: ampicillin, 1 g; gentamicin, 80 mg
- Review all radiographs and determine whether bowel loops lie anterior to bladder.
- Place Foley catheter to distend bladder with saline
- Local anesthesia with at least 10 mL lidocaine (Xylocaine)
- Make a skin incision which is approximately two times the diameter of the Foley catheter within the skin.
- Using a metallic trocar which fits around a 14-Fr or 16-Fr Foley catheter, insert the metallic trocar into the bladder under direct US guidance. Make sure that the device is well lubricated with lubricating jelly before insertion.
- Inflate the Foley balloon and peel the Foley catheter off the trocar. Inject the Foley catheter to confirm the position within the bladder.
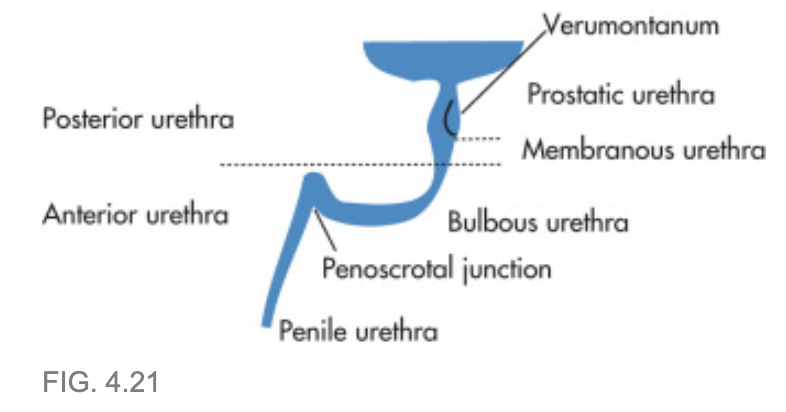
What comprises the posterior urethra?
Posterior urethra = prostatic + membranous portions

What comprises the anterior Urethra?
• Anterior urethra = bulbous and penile portions
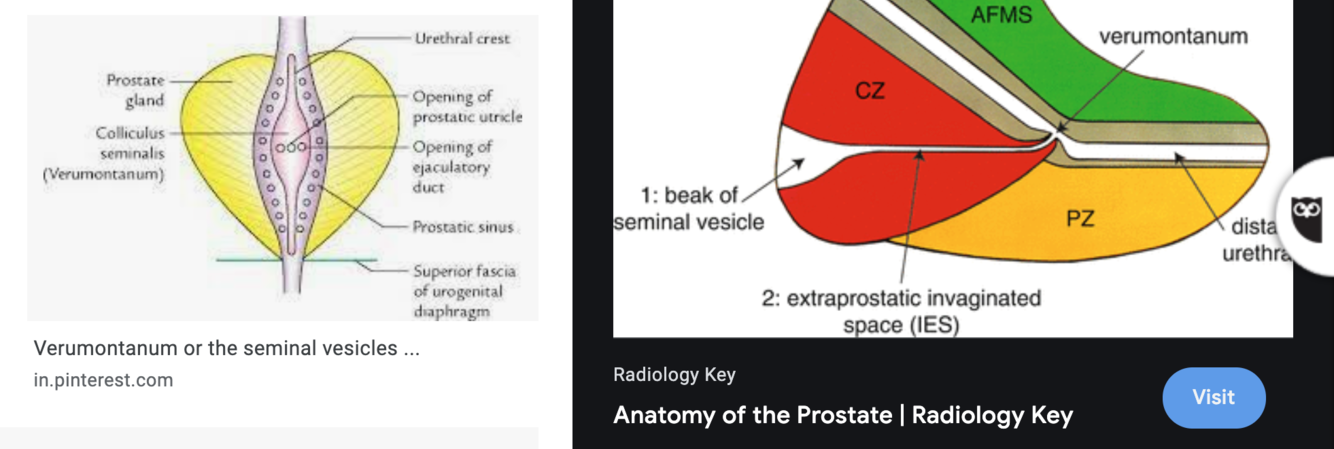
What is this?

- Verumontanum:
- dorsal elevation in prostatic urethra
- receives
- paired ejaculatory ducts and the
- utricle
- Verumontanum is a structure located on the floor of the posterior urethra, which marks the boundary between the membranous and the prostatic segment. During endoscopic resections, it represents a landmark of the striated sphincter and, implicitly, of the lower limit of the intervention. Usually it has a length of 15–17 mm and a height of 3 mm, although there are numerous variations of both shape and size. On both sides of the urethral ridge, the orifices of the prostatic ducts open, and the ejaculatory ducts orifices and prostatic utricle orifice can be found on the upper edge.
- https://www.sciencedirect.com/science/article/pii/B9780128024065000124
What does the membranous urethra demarcate?
Membranous urethra demarcates urogenital diaphragm;
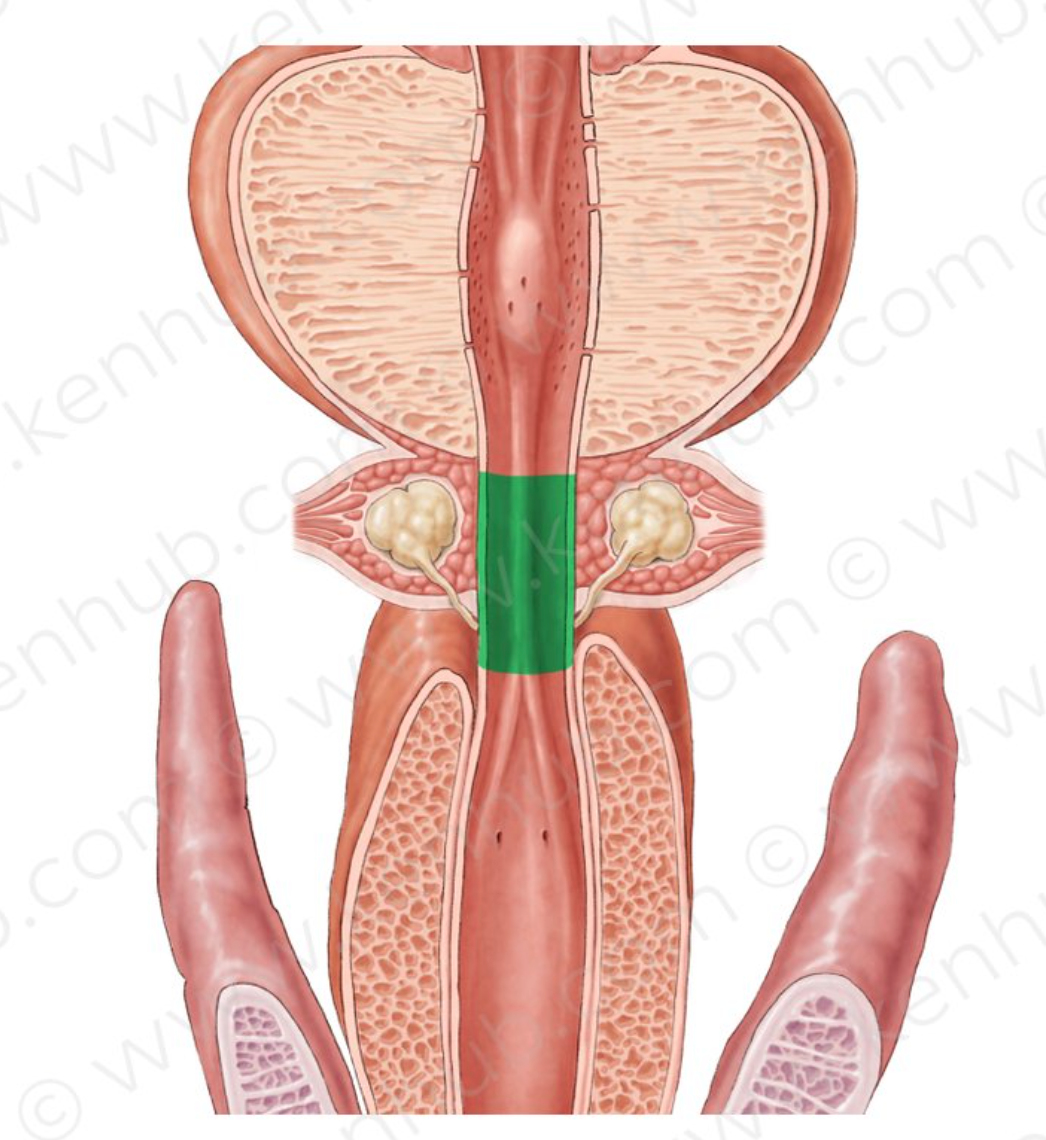
What is the membranous urethra radiographically defined as?
radiographically defined as the portion between the distal verumontanum and the cone of bulbous urethra
Where do the bulbourethral glands drain into?
What are they AKA?
Cowper glands in urogenital diaphragm; ducts empty into proximal bulbous urethra

What are the labeled structures?

A. Utricle
B. Prostatic urethra
Utricle: müllerian duct remnant; blind-ending pouch in midline
https://caps.nationwidechildrens.org/radiology/atlas/Urethra_Atlas/Prostatic_utricle.html
The prostatic utricle is a small, epithelium-lined diverticulum of the prostatic urethra. It is located in the verumontanum between the two openings of the ejaculatory ducts and extends backward and slightly upward for a very short distance within the medial lobe of the prostate.
It is a normal anatomic variant representing the remnant of the fused caudal ends of the Müllerian ducts, and thus is the homolog of the female vagina and uterine cervix.
When there is deficient secretion or resistance to Müllerian inhibitory factor (MIF), there is failure of normal fusion of the urogenital folds resulting in hypospadius. Hypospadius has the most common association with the prostatic utricle, with an estimated incidence of 14-47%. In the absence of other Müllerian duct derivatives (fallopian tubes, uterus and upper vagina), hypospadius and utricular enlargement are not indicative of an intersex condition. The increasing severity of the hypospadius correlates with increasing size of the utricle. A utricle not uncommon in prune-belly syndrome, and may be seen in patients with imperforate anus and recto-urethral fistula, and in patients with Down syndrome.
The prostatic utricle distends with urine during voiding and then passively drains. Poor emptying leads to urine retention and stasis. Stone formation may result from obstruction. Patients present clinically with chronic urinary tract infection, hematuria, urethral discharge, epididymitis and voiding dysfunction.
The normal prostatic utricle is occasionally seen as an incidental finding on routine VCUG as a tiny diverticulum of a few millimeters in length or on rare occasions measuring up to 1 cm or more. A large prostatic utricle is more often associated with male hypospadius. VCUG and retrograde urethrography (RUG) define the utricular size and its origin from the prostatic urethra. Occasionally a prostatic utricle is bifid, reflecting the bifid nature of its precursors, namely the paired Müllerian ducts. In patients with a large prostatic utricle, direct catheterization of the bladder during VCUG may be difficult secondary to preferential passage into the utricle. Facilitation of catheter placement into the bladder can be accomplished with use of a Coude’ catheter with the tip directed anteriorly, direct perineal pressure and/or insertion of a finger in the rectum with upward pressure during catheter placement.
Differential Diagnosis
- Ectopic ureter. 2. Dilated ejaculatory duct. 3. Mullerian duct cyst.
- Extravasation




















-
CHEST IMAGING 1100
-
CHEST IMAGING 2100
-
CHEST IMAGING 343
-
CHEST IMAGING 4 (TUMOURS)81
-
CHEST IMAGING 5 PATHOLOGY2
-
CARDIAC IMAGING 1100
-
CARDIAC IMAGING 2100
-
CARDIAC IMAGING 3100
-
CARDIAC IMAGING 443
-
GIT 1101
-
GIT 2100
-
GIT 3100
-
GIT 4102
-
Hepatobilary155
-
Biliary System76
-
Pancreas66
-
Spleen24
-
Adrenal Glands70
-
GENITOURINARY IMAGING 197
-
GENITOURINARY IMAGING 2100
-
GENITOURINARY IMAGING 3100
-
GENITOURINARY IMAGING 4100
-
GENITOURINARY IMAGING 545
-
RETROPERITONEUM33
-
Male Pelvis10
-
GIT PATHOLOGY31
-
Skeletal Dysplasias18
-
MSK104
-
MSK Crack the Core70
-
MSK 295
-
MSK 3100
-
Neuro100
-
Neuro 222
-
NEURO 375
-
Head and Neck 1100
-
Head and Neck 2100
-
Head and Neck 3100
-
Head and Neck 4100
-
Head and Neck 555
-
DDX Head and Neck35
-
Vascular10
-
IR30
-
BREAST IMAGING52
-
OBSTETRICS17
-
GYNAECOLOGY40
-
PAEDIATRICS 196
-
PAEDIATRICS 297
-
PAEDIATRICS 395
-
Nuclear Medicine 134
-
PET CT16
-
Syndromes94
-
HAEMATOLOGY6
-
PATHOLOGY 141
-
Crack the core WHen I Say you say...489
-
Physics31
-
crack the core exam case companion18
-
EPONYMOUS Diseases/signs22
-
What the F&^# is that word?10
-
Radiology Signs25
-
Mnemonics36
-
GIT Pathology1
-
NEURO MRI PHYSICS14
-
GREAT CHEST XRAY CASES1
-
THIS PATIENT IS TYPICAL OF X CONDITION2
