What is a Rathke Cleft Cysts?
AKA?
Where is it found?
T1 and T2 features?
Pathognomic sign?
- AKA: Pars intermedia Cysts (if small and asymptomatic)
- non-neoplastic
- sellar or supra sellar epithelium-line cysts arising from the embryologic remant
- well defined non-enhacing midline cyst within the sella arising between the anterior and intermediate lobes of the pituitary.
- 40% are purely intrasellar
- 60% have supra sella extension.
- Purely suprasellar location, although reported, is rare.
- T1 = 50% hyper (secondary to high protein content), 50% hypo
- T2 = 70% are hyperintense, 30% are iso or hypointense.
- T1 C+ = no contrast enhancement of the cyst is seen.
- 75% of cases a small non-enhancning intracystic nodule can be identified which is virtually pathognomoic of a Rathke cleft cyst.
What is the dx?
What are 5 causes?
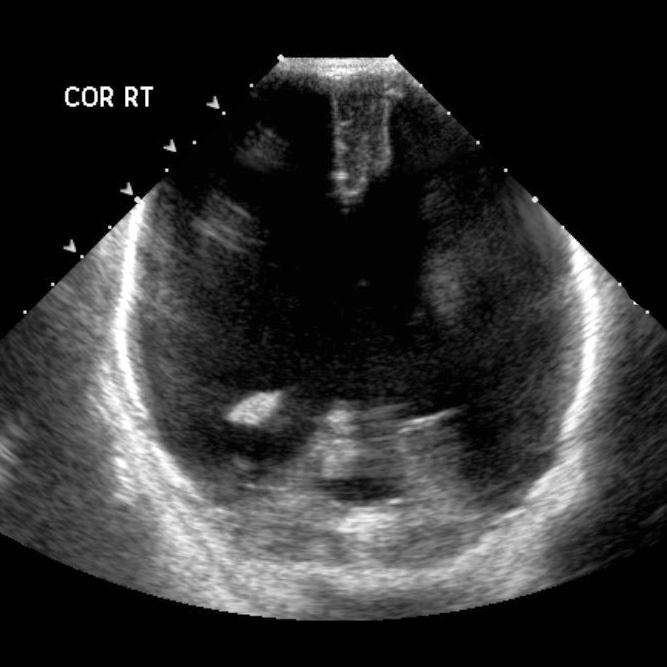
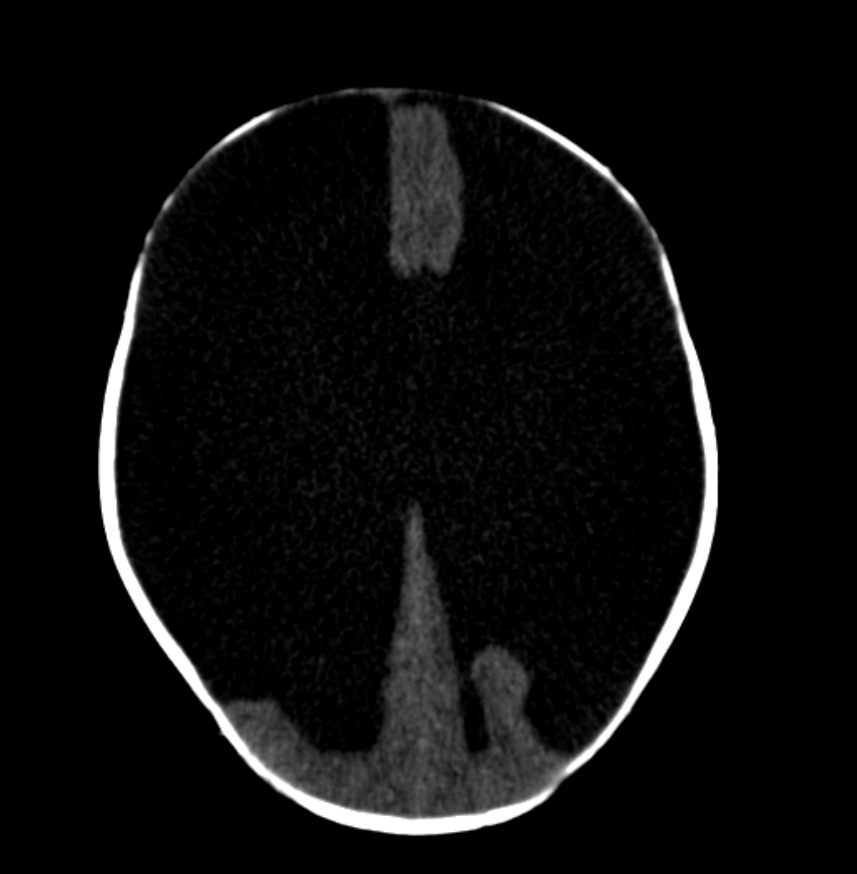
Hydraencephaly
Hydranencephaly is a rare encephalopathy that occurs in-utero. It is characterised by destruction of the cerebral hemispheres which are transformed into a membranous sac containing cerebrospinal fluid and the remnants of cortex and white matter 1. Porencephaly is considered a less severe degree of the same pathology 10
Five aetiologies have been described:
- infarction: bilateral occlusion of the supraclinoid segment of the internal carotid arteries or of the middle cerebral arteries 3
- leukomalacia: an extreme form of leukomalacia formed by confluence of multiple cystic cavities 4
- diffuse hypoxic-ischaemic brain necrosis: fetal hypoxia due to maternal exposure to carbon monoxide or butane gas may result in massive tissue necrosis with cavitation and resorption of necrotised tissue 1
- infection: necrotising vasculitis or local destruction of the brain tissue secondary to intrauterine infection, e.g. congenital toxoplasmosis, cytomegalovirus, and herpes simplex(HSV) infections 1,8
- thromboplastic material from a deceased co-twin monochorionic twins have presented with a variety of cerebral lesions. lesions in the recipient twin result from emboli or thromboplastic material originating from the macerated co-twin 4
Case Discussion
There is marked enlargement of fluid spaces with little if any overlying cerebral parenchyma except for the posterior fossa and para medial location along the falx.
The posterior fossa structures are inferiorly displaced and the fourth ventricle is not well seen. Higher cuts demonstrate marked cerebral destruction of both cerebral hemispheres predominately in the distribution mid cerebral arteries with minimal residual tissue identified both anteriorly and posteriorly. The anterior fontanelle is bulging.
This case demonstrates typical CT and ultrasound appearances of hydranencephaly, which is in almost all cases not compatible with significant post natal survival.
https://radiopaedia.org/cases/hydranencephaly-1?lang=us
What is this?
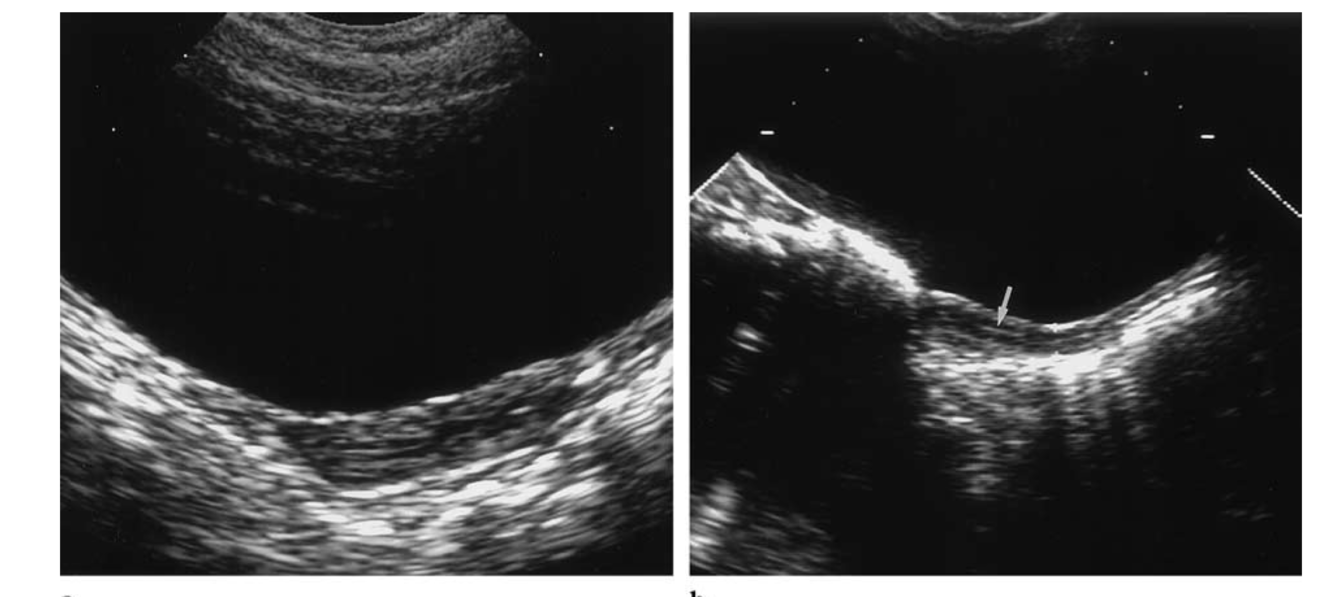
Uterus
What are US prepubertal features of the Uterus
The prepubertal uterus has a tubular configuration (AP cervix equal to AP fundus) or sometimes a spade shape (AP cervix larger than AP fundus).
The endometrium is normally not apparent; however, high-frequency transducers can demonstrate the central lining.
The length is 2.5–4 cm; the thickness does not exceed 10 mm.
https: //pubs.rsna.org/doi/pdf/10.1148/radiographics.21.6.g01nv041393
* Figure 2. Prepubertal uterus. (a) Longitudinal US scan obtained in a 5-year-old girl shows a tubular uterus; the anteroposterior diameter is 6 mm. (b) Longitudinal US scan obtained in a 6-year-old girl shows the endometrial lin- ing as a thin echogenic line (arrow).*
- LUL colapse causes in kids
- FB
- endobronchia lesion -> carcinoid
- mucous plug
Three facts about Crossed Renal Ectopia
- 1/1000
- M:F 2:1
- 90% are fused.
What is the incidence of Congenital diaphragmatic hernia (CDH)?
What is the mortality rate?
What is the most reliable predictor of post natal survival?
What are the clinical symptoms?
What are 3 associated anomalies?
- Incidence: 1/2000-3000 births.
- Mortality rate: isolated hernias is 60%.
- Higher when other abnormalities are present.
- Most reliable predictor of postnatal survival is absence of liver herniation.
- Respiratory distress occurs in neonatal period.
- Associated abnormalities include:
- Pulmonary Hypoplasia
- CNS abnormalities.
- NTDs
- Anencephaly.
What is this?
What sequence should you ask for?
What is it associated with clinically?
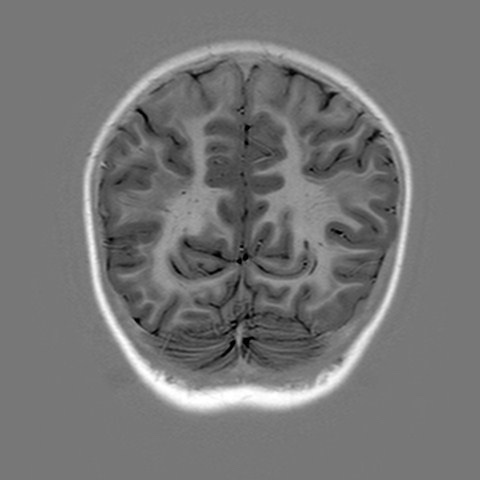
Band Heterotopia
Ask for:
- Inversion Recovery Sequence
- A/W seizures
Case courtesy of Dr Ian Craven, Radiopaedia.org, rID: 78613
What is the modality of choice for DDH and why?
- USS is the modality of choice prior to the ossification of the proximal femoral epiphysis.
- Once there is a significant ossificaiton then an xray is required.
- USS is the test of choice in <6 months as the proximal femoral epiphysis has not yet signficantlly ossified.
- Real time dynamic examinatio allowing the stability of the hip to the assessed with stress views.
3 types of Pulmonary Hypoplasia
- agenesis:
- complete absence of one or both lungs.
- agenesis:
- Aplasia:
- abscence of lung except for a rudimentary bronchus that ends in a blind pouch.
- Aplasia:
- -Hypoplasia:
- decrease in the number and size of airways and alveoli: hypoplastic PA.
What is the rule for assessing Splenomegally in paediatric patients?
Max splenic size (cm)
- 1/2 Pts age +6
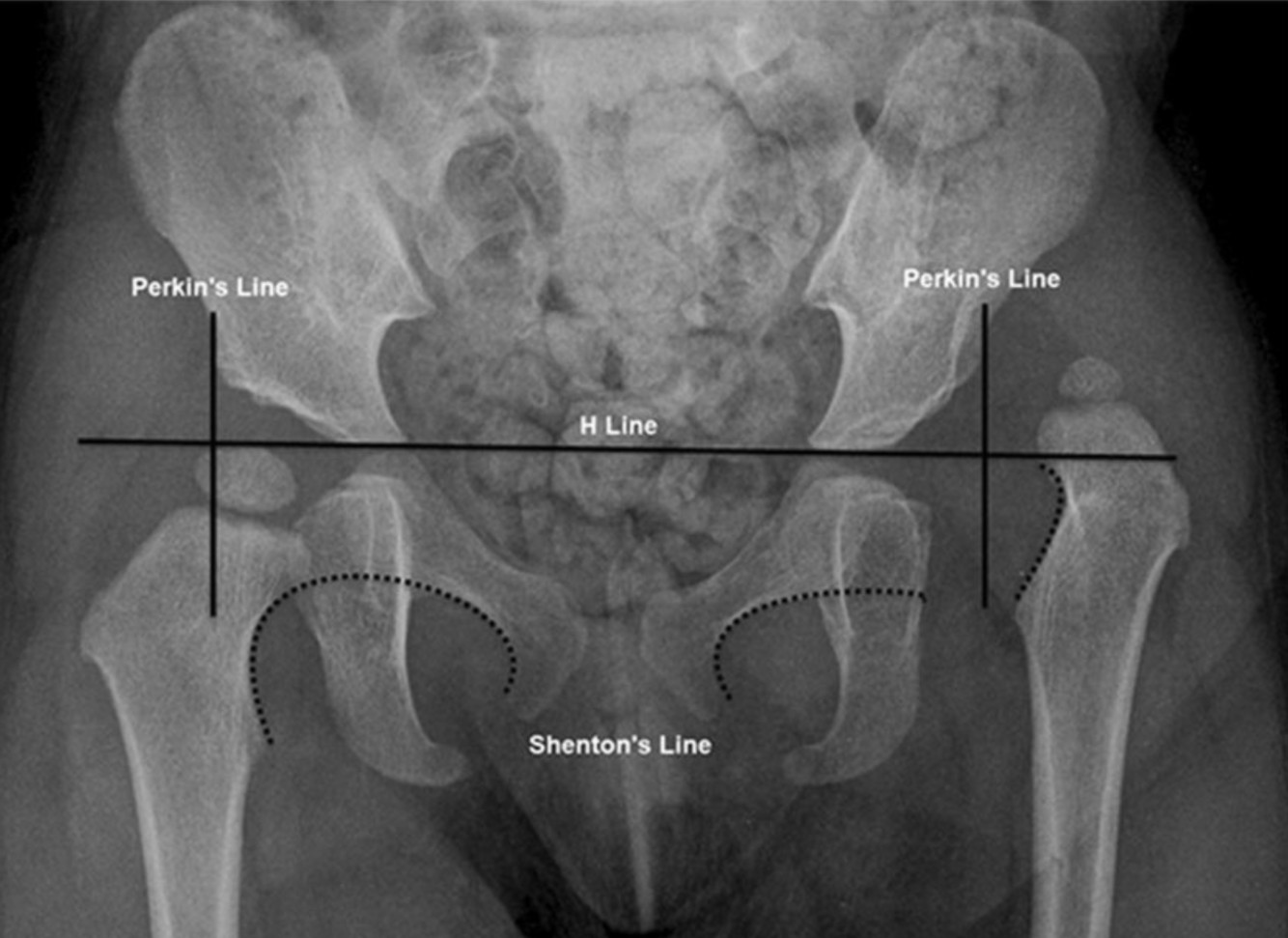
What is the Hilgenreiner line?
- Drawn horizontally through the superior aspect of both triradiate cartilages.
- It should be horizontal but is mainly used as a reference for the Perkin line
- Measurment of the acetabular angle
The Perkins line and Shenton arc on radiography. Anteroposterior radiograph in a 2-year-old girl with left developmental dysplasia of the hip. The Perkins line is drawn perpendicular to the Hilgenreiner line (H line) and intersects the lateral acetabular rim. The Shenton arc is formed by the medial cortex of the femoral neck and the inferior cortex of the superior pubic ramus (dotted lines). The normal right hip shows the femoral head confined to the inferomedial quadrant and a continuous Shenton arc. The abnormal left hip shows the dislocated femoral head within the superolateral quadrant and a discontinuous Shenton arc
https://www.researchgate.net/figure/The-Perkins-line-and-Shenton-arc-on-radiography-Anteroposterior-radiograph-in-a_fig10_337009090
What is Laryngomalacia?
Clinical symptoms?
When does it occur?
How do you diagnose it?
- Common cause of stridor in the first year of life.
- Immature laryngeal cartilage leads to supraglottic collapse during inspiration.
- Stridor improves with activity and is relieved by propositions or neck extension.
- Self-limited course.
- diagnosis is established by fluoroscopy where there is laryngeal collapse with inspiration.
Etiology: congenital cartilage abnormality in larynx
Imaging: dynamic partial supraglottic collapse of the larynx during breathing
https://pediatricimaging.org/diseases/laryngomalacia/
Which has normal Pulmonary Blood flow on CXR?
- VSD
- TOF
- AP window
- PDA
- Coarctation
(Paeds tute 10.9.20)
Co-arctation
- PDA > L-> R Shunt -> Plethoric
- VSD > L-> R Shunt -> Plethoric
- TOF -> oligaemic
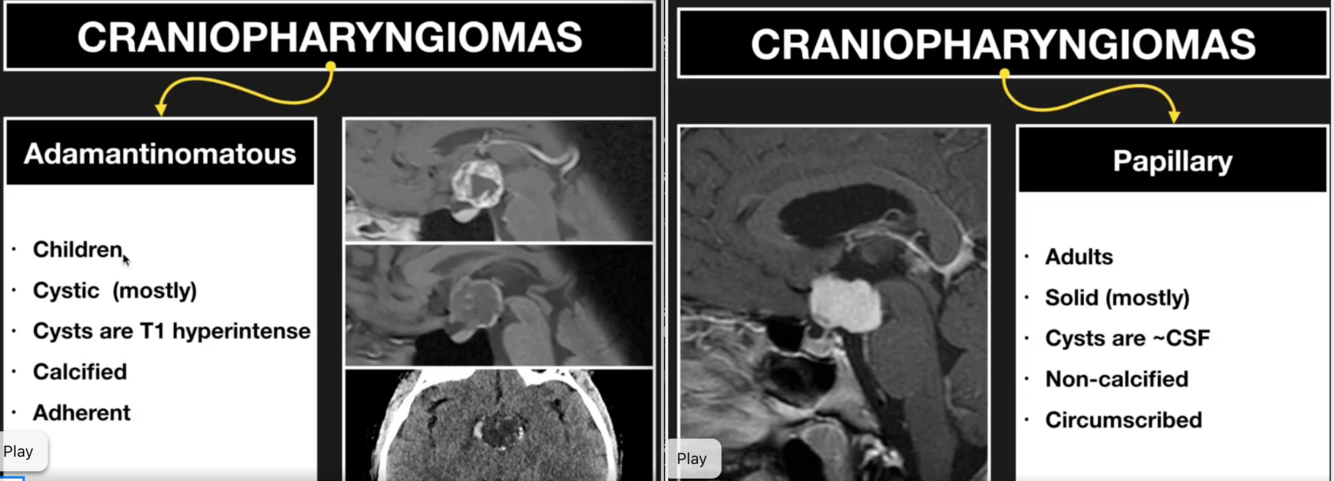
What is a Craniopharyngioma?
- intro
- relatively benign neoplasms that typically arise in the sellar/suprasellar region.
- 1-5% of primary brain tumors and can occur anywhere along the infundibulum, from the floor of the 3rd ventricle to the pituitary gland.
- bimodal distribution 5-15years (adamantinomatous)
- 40 years (both papillary and adamantinomatous)
- no gender predilection.
- Subtypes
- adamantinomatous (more common)
- papillary
- mixed/transitional (imaging and prognosis similar to adamantinomatous).
- Ddx
- Intracranial teratoma
- presence of fat is helpful but requires fat sat sequences or CT to confirm
- Pituitary macroadenoma
- can look very similar
- usually has intrasellar epicenter with pituitary fossa enlargement rather than the suprasellar epicenter
- don’t usually calcify
- Rathke cleft cyst
- no solid or enhancing component
- calcification is rare
- unilocular
- the majority are completely or mostly intrasellar.
- https://www.facebook.com/watch/?v=557576101663321
- Intracranial teratoma
Wolffian Duct
- anlage for vas deference, seminal vesicles, epididymis
- guides ureteral migration to the bladder.
- induces kidney development and ascent
- induces Mullerian duct development in females.
Name the following vascular rings.
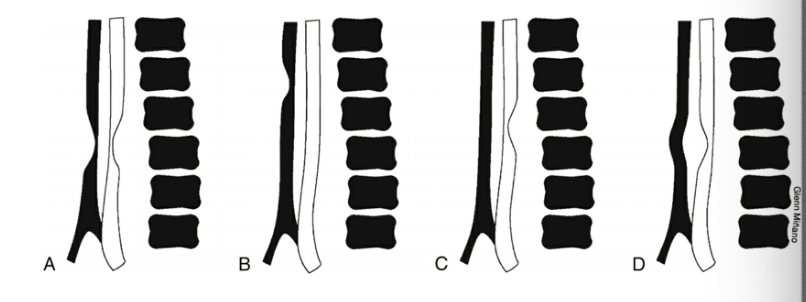
- Double aortic arch
- Innominate artery compression
- Left arch with aberrant right subclavian artery. or right arch with abberant left subclavian artery.
- Aberrant lefft pulmonary artery (pulmonary sling)
LCH Extraskeleta manifestations
Pulmonary Involvement
alveolar disease (exudate of histiocytes)
interstitial pattern (upper lobe pred)
CNS
meningeal involvement
pituitary
RES organs
Liver, spleen, LNS
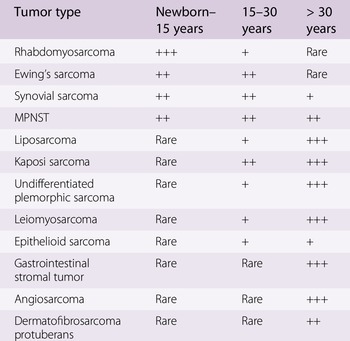
12 Paediatric Soft tissue tumours
- Rhabdomyosarcoma
- Ewings Sarcoma
- Synovial Sarcoma
- MPNST
- Liposarcoma
- Kaposi Sarcoma
- Undifferentiated pleomorphic sarcoma
- Leiomyosarcoma
- Epitheliod Sarcoma
- GIST
- Angiosarcoma
- Dermatofibrosarcoma Proteuberans
CHARGE SYNDROME
Which gene?
What are the main characteristics?
CHARGE syndrome is a phenotype associated with CHD7 gene mutation originally defined by a constellation of congenital anomalies:
- C: coloboma
- H: heart defects
- A: atresia choanae
- R: retarded growth and development
- G: genital hypoplasia
- E: ear abnormalities and/or deafness
According to updated diagnostic criteria, the most defining features are the 4 C’s:
- coloboma
- choanal atresia
- cranial nerve anomalies (especially olfactory pathway absence)
- characteristic ear anomalies (especially semicircular canal dysplasia/aplasia)
- Epidemiology
- The incidence is 1-12 per 100,000 births 6.
- Clinical presentation
- CHARGE syndrome is usually suspected at birth once multiple congenital abnormalities are identified.
- Diagnosis
- The diagnosis of CHARGE syndrome can be made on clinical grounds 6,11:
- definite CHARGE syndrome: 4 major characteristics or 3 major plus 3 minor characteristics
- possible/probable CHARGE syndrome: one-to-two major characteristics and several minor characteristics
- Major criteria
- coloboma (80%): ranges from defect of iris, retina, choroid, or disc, to microphthalmia or anophthalmia
- choanal atresia/stenosis (45%) or cleft palate (25-50%)
- cranial nerve anomaly/dysfunction
- olfactory (90%): hyposmia/anosmia
- facial (40%): facial palsy
- vestibulocochlear (95-100%): sensorineural deafness
- glossopharyngeal or vagal (60-80%): velopharyngeal incoordination for suck/swallow
- characteristic ear anomalies (some or all of the following) (90%)
- abnormal auricle: short and wide (lop/cup shaped), absent lobule, truncated helix, prominent antihelix
- ossicular malformations
- Mondini malformation
- absent/hypoplastic semicircular canals
- Mondini malformation
- Minor criteria
- urogenital abnormalities
- kidney
- duplex kidney
- renal hypoplasia/solitary kidney
- penis
- hypospadias
- penile agenesis
- scrotum/testes
- bifid scrotum
- cryptorchidism
- vaginal atresia
- uterine atresia
- congenital heart disease
- tetralogy of Fallot
- atrioventricular canal defect
- double outlet right ventricle
- short stature
- cleft palate +/- lip
- esophageal atresia / tracheo-esophageal fistula (~15%) 2
- characteristic facies
- developmental delay
- urogenital abnormalities
- Pathology
- CHARGE syndrome is thought to occur due to a disturbance in embryonic differentiation ~35th to 45th day of gestation.
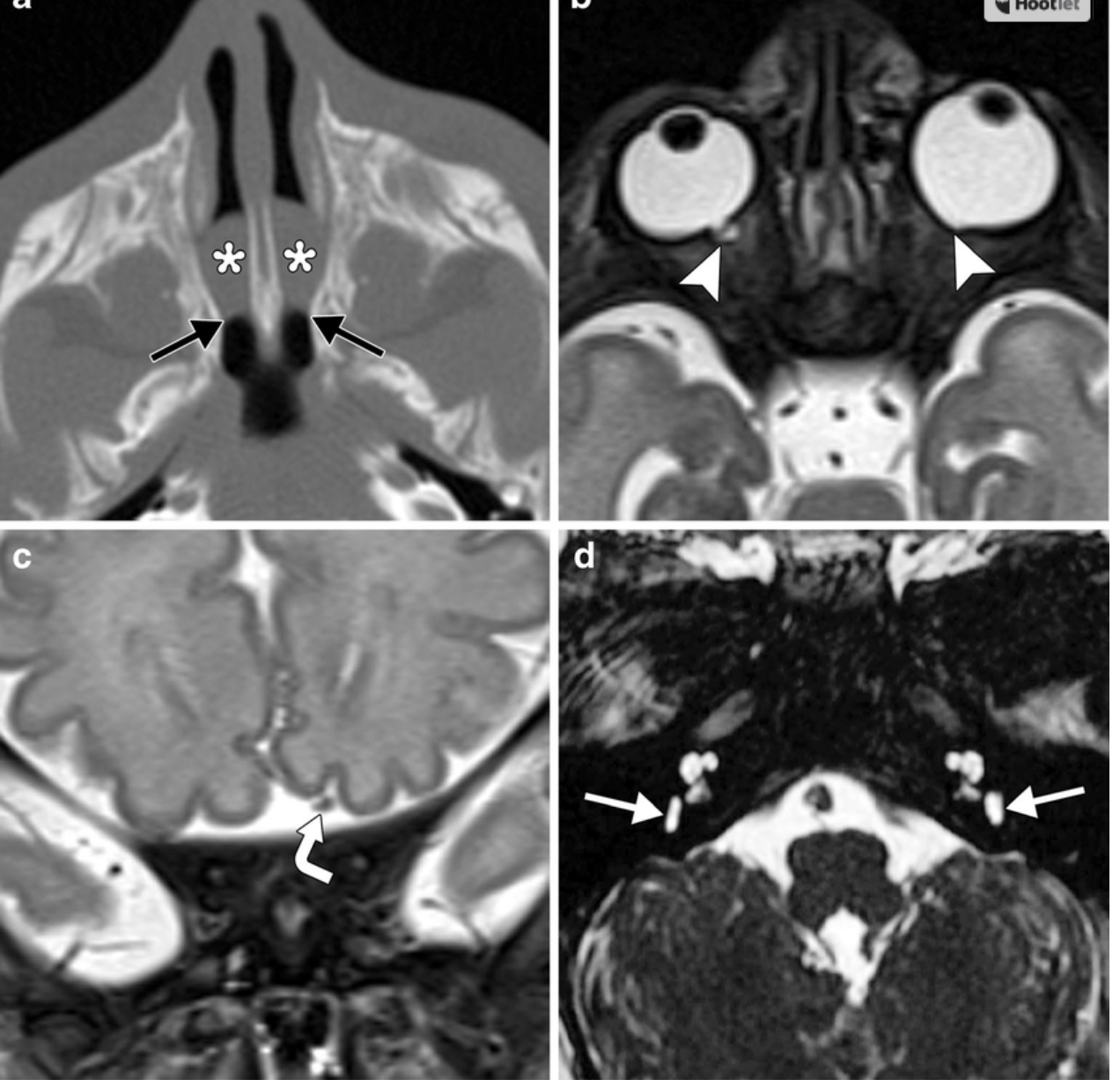
CHARGE syndrome. Axial CT image in a 6-day-old boy (a) shows bilateral bony and membranous choanal atresia with a thickened vomer and medial deviation of the lateral nasal walls at the level of the choanae (black arrows). There are secretions layering within the nasal cavities (*). Axial T2-weighted MRI at 4 days of age (same patient) (b) shows bilateral colobomas (arrowheads). Coronal T2weighted MRI (c) shows that the olfactory apparatus is absent on the right, but intact on the left (curved arrow). Axial CISS (constructive interference in steady state) image (c) shows bilateral absent semicircular canals and hypoplastic vestibules (white arrows). There is also bilateral cochlear nerve aperture and internal auditory canal stenosis
https://www.researchgate.net/figure/CHARGE-syndrome-Axial-CT-image-in-a-6-day-old-boy-a-shows-bilateral-bony-and_fig8_270650182
Causes of nephrocalcinosis
Cortical: “COAG”
- Renal cortical necrosis
- Oxalosis
- Alport syndrome
- (chronic) glomerulonephritis
Medullary:
- deposition of calcium salts in the medulla of the kidney.
- Causes “HAM HOP”
- hyperparathyroidism
- renal tubular Acidosis
- Medullary sponge kidney
- Hyper or hypo thyroidism
- Oxalosis
- papillary necrosis
- Hypervitaminosis D.
- Milk alkali syndrome
- Sarcoid
-year-old male presents with hematuria. An MRI scan was performed. Axial and coronal T2-weighted images are shown.
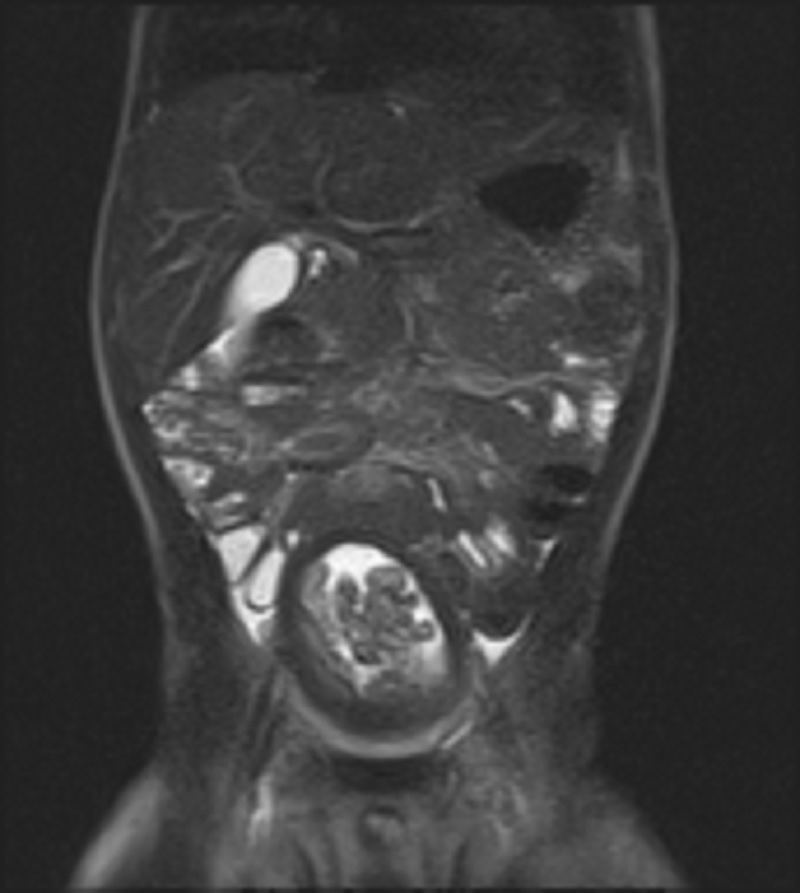
There is a polypoid mass in the bladder. The grape-like appearance is characteristic of the botryoid type of rhabdomyosarcoma. Rhabdomyosarcomas are the most common malignant bladder masses in the pediatric population.
Paragangliomas of the bladder may have a similar appearance with a macrolobulated appearance and T2-hyperintense signal, but they are more often seen in patients ages 30 to 60. Hemangiomas are often seen in the setting of other vascular malformations and are similar in appearance to hemangiomas seen elsewhere. Cystitis glandularis may present as nodules on a background of diffuse bladder wall thickening. Bladder neurofibromas are rare and may demonstrate a target appearance on T2-weighted imaging, with central low signal and peripheral high signal.
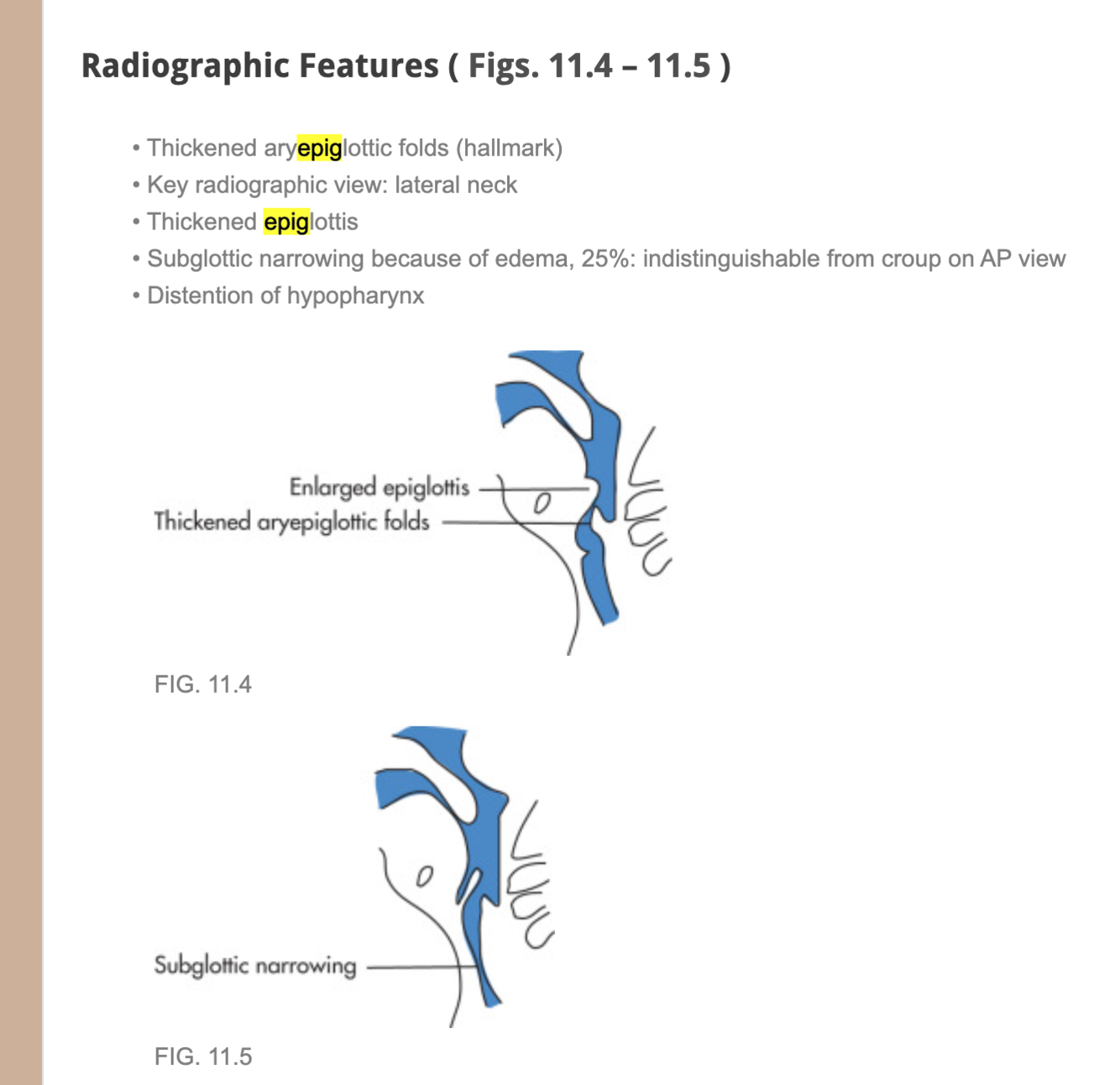
Epiglottitis
- bacterial infection of the upper airway by H influenza
- 3-6 years old
- Rtx with prophylactic intubation for 24-48 hours and antibiotics
- fever, dysphasia, drooling, sore throat
- X-ray: thickened aryepiglottic folds, lateral view: thickened epiglottis, subglottic narrowing because of edema
- 25% indistinguishable from croup on AP view.
- Distension of hypopharynx.
Tracheal stenosis
Three types:
- diffuse Hypoplasia (30%)
- Focal ring like stenosis (50%)
- Funnel like stenosis (20%)
Rathke Cleft Cysts
- AKA: Pars intermedia Cysts (if small and asymptomatic)
- non-neoplastic
- sellar or supra sellar epithelium-line cysts arising from the embryologic remants
- well defined non-enhacing midline cyst within the sella arising between the anterior and intermediate lobes of the pituitary. 40% are purely intrasellar and 60% have supra sella extension. Purely suprasellar location, although reported, is rare.
- T1 = 50% hyper (secondary to high protein content), 50% hypo
- T2 = 70% are hyperintense, 30% are iso or hypointense.
- T1 C+ = nocontrast enhancement of the cyst is seen.
- 75% of cases a small non-enhacning intracystic nodule can be identified which is virtually pathognomoic of a rathke cleft cyst.






















-
CHEST IMAGING 1100
-
CHEST IMAGING 2100
-
CHEST IMAGING 343
-
CHEST IMAGING 4 (TUMOURS)81
-
CHEST IMAGING 5 PATHOLOGY2
-
CARDIAC IMAGING 1100
-
CARDIAC IMAGING 2100
-
CARDIAC IMAGING 3100
-
CARDIAC IMAGING 443
-
GIT 1101
-
GIT 2100
-
GIT 3100
-
GIT 4102
-
Hepatobilary155
-
Biliary System76
-
Pancreas66
-
Spleen24
-
Adrenal Glands70
-
GENITOURINARY IMAGING 197
-
GENITOURINARY IMAGING 2100
-
GENITOURINARY IMAGING 3100
-
GENITOURINARY IMAGING 4100
-
GENITOURINARY IMAGING 545
-
RETROPERITONEUM33
-
Male Pelvis10
-
GIT PATHOLOGY31
-
Skeletal Dysplasias18
-
MSK104
-
MSK Crack the Core70
-
MSK 295
-
MSK 3100
-
Neuro100
-
Neuro 222
-
NEURO 375
-
Head and Neck 1100
-
Head and Neck 2100
-
Head and Neck 3100
-
Head and Neck 4100
-
Head and Neck 555
-
DDX Head and Neck35
-
Vascular10
-
IR30
-
BREAST IMAGING52
-
OBSTETRICS17
-
GYNAECOLOGY40
-
PAEDIATRICS 196
-
PAEDIATRICS 297
-
PAEDIATRICS 395
-
Nuclear Medicine 134
-
PET CT16
-
Syndromes94
-
HAEMATOLOGY6
-
PATHOLOGY 141
-
Crack the core WHen I Say you say...489
-
Physics31
-
crack the core exam case companion18
-
EPONYMOUS Diseases/signs22
-
What the F&^# is that word?10
-
Radiology Signs25
-
Mnemonics36
-
GIT Pathology1
-
NEURO MRI PHYSICS14
-
GREAT CHEST XRAY CASES1
-
THIS PATIENT IS TYPICAL OF X CONDITION2
