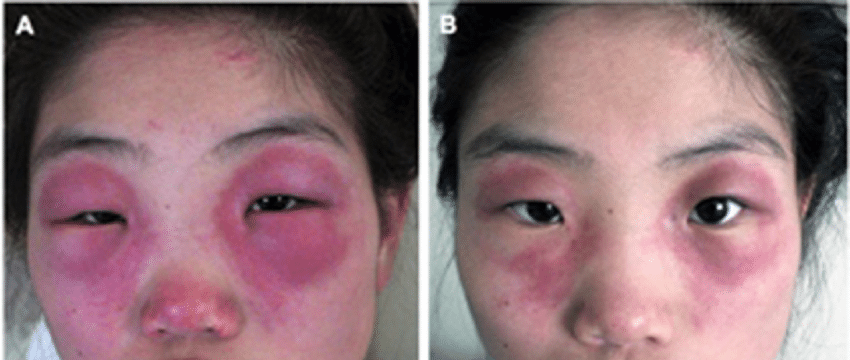
Heliotrope rash
Bluish-purple discoloration on the face, eyelids, neck, shoulders, upper chest, elbows, knees, knuckles, and back of patients with dermatomyositis
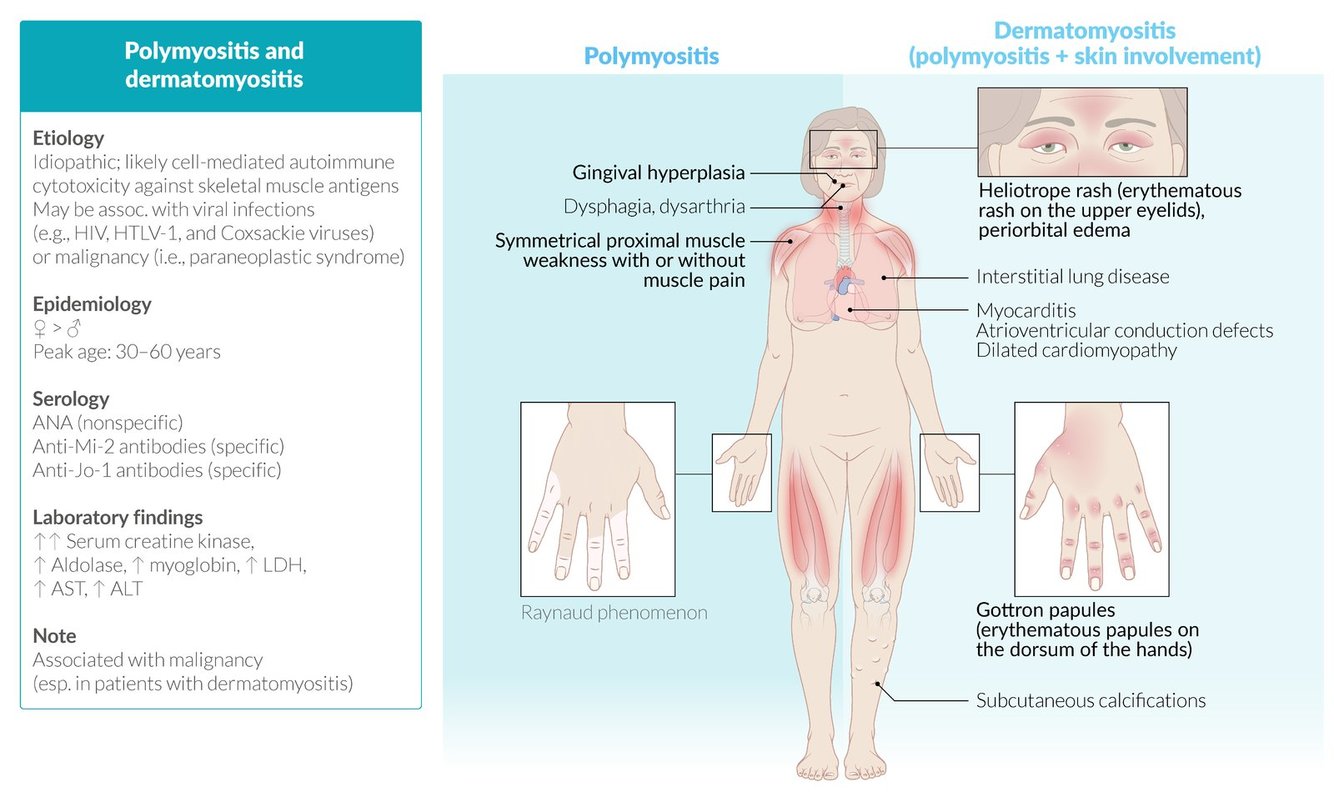
Polymyositis and dermatomyositis comparison
Grotton nodules
Flat-topped, raised, nonpruritic lesions found over the dorsum of the MCP, PIP, and DIP in dermatomyositis/polymyositis
Pathology shows acanthosis and papillomatosis

Anti-Jo1
Antibody that recognizes cytoplasmic histidyl transferase RNA synthetase
Polymyositis
- Onsets in the late teens-early twenties over the course of ~3-6 months
- Often occurs with Sjogren’s syndrome or Rheumatoid arthritis
- Clinical features: Proximal muscle pain and weakness, dysphagia, dyspnea, hoarseness/dysphonia
- Note: Dysphagia is more common with polymyositis than dermatomyositis
- Exam features: Fine pulmonary rales, heart block/bradyarrhythmia, muscle tenderness
Dermatomyositis
- Onsets age 40-50 over the course of days to weeks
- Clinical features: Proximal muscle pain and weakness, dysphagia, dyspnea
- Exam features: heliotrope rash, grotton papules, fine pulmonary rales, heart block/bradyarrhythmia, muscle tenderness
EKG abnormalities in polymyositis/dermatomyositis
- Left anterior fascicular block
- Right bundle-branch block
- Heart block
Historical symptoms of proximal muscle weakness
Upper extremity: Exhaustion with brushing teeth, dropping objects, difficulty reaching overhead
Lower extremity: Difficulty walking up stairs, difficulty rising from a seated position, using arm-rests to aid in standing from a seated position
“Shawl sign”
Describes the wrapping of the heliotrope rash around the neck, shoulders, and upper back with relative sparing of the lower chest and lower back

Calcinosis cutis
Seen in children with dermatomyositis
Development of dystrophic calcification in the softtissues and muscles, leading to skin ulcers, secondary infection, and joint contractures
Occurs less commonly in adults.

Inclusion body myositis
- Presents more commonly in male patients age ~60 years over the course of years
- Often asymmetrical, and also affects distal muscles
- This is a hugely imporant differentiating factor from PM/DM
- Atrophy of the deltoids and quadriceps is often present
- Peripheral neuropathy with loss of DTRs can be present in some patients
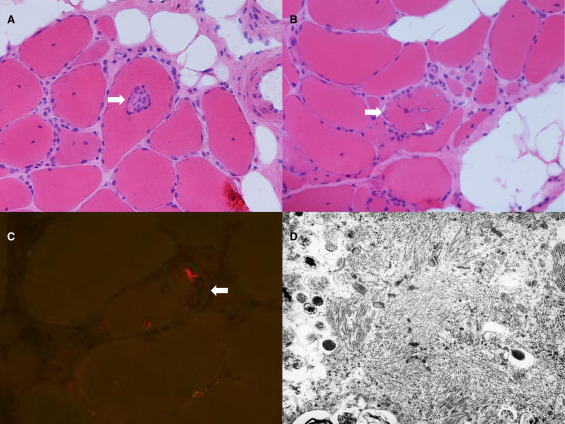
- Pathology shows inclusion bodies within muscle and diffuse lymphocytic infiltration (shown)
Generally speaking, the definitive diagnosis for any myopathy is ___
Generally speaking, the definitive diagnosis for any myopathy is muscle biopsy
Polymyositis and dermatomyositis you can get away with just demonstrating the presence of specific antibodies, if they are present
Diagnosis of inclusion body myositis
- Clinical characteristics
- Asymmetrical proximal and distal muscle weakness (typically involving the deltoids and quadriceps)
- Lab findings:
- Elevated CK (600-800, sometimes normal)
- Elevated ESR, CRP
- Autoantibodies:
- anti-Mup44
- Definitive diagnosis: EMC-NCS followed by biopsy
Diagnosis of polymyositis/dermatomyositis
- Both are, to some degree, diagnoses of exclusion
- Clinical characteristics
- Proximal muscle weakness
- Raynaud’s phenomenon
- Rash
- Lab findings:
- Elevated CK (1,000 - 10,000)
- Elevated ESR, CRP
- Associated autoantibodies:
- anti-Jo1
- anti-PL-7
- anti-PL-12
- anti-OJ
- anti-EJ
- Definitive diagnosis:EMC-NCS followed by biopsy
Selecting a muscle to biopsy for suspected myositis syndrome
Should be an atrophied muscle that is likely to demonstrate the pathologic features of end-stage disease
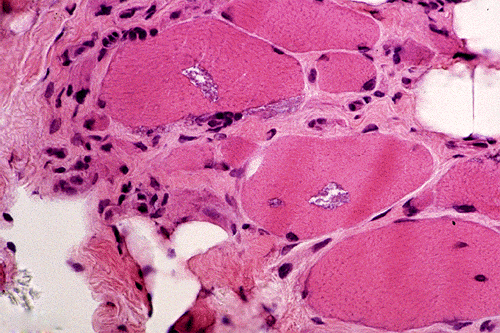
Pathologic hallmarks of inclusion body myositis
- Eosinophilic cytoplasmic inclusions
- Vacuoles rimmed with basophilic granules
- Foci that stain Congo red (amyloid)
- On electron microscopy: cytoplasmic helical filaments that contain beta-amyloid
Drugs which may induce inflammatory myopathies
- Statins (may be directly metabolic OR may be via anti-HMGCoaR)
- Penicillamine (for Wilson’s disease, soluble copper chelator)
- Ziduvodine (HIV RTI)
Polymyositis and dermatomyositis biopsies
Show chronic inflammation and complement deposition
Treatment of polymyositis/dermatomyositis/IBM
- Induction: 4-6 weeks of prednisone
- Maintenance: Methotrexate or azathioprine
- Refractory cases: Add IVIg
- Screening: CXR, PFTs, EKG
- If a paramalignant etiology of PM/DM is suspected, CT chet/abd/pelvis is indicated to screen for malignancy. Clinical suspicion for malignancy should remain high for the next few years following diagnosis even if the imaging is negative.
- Rehab: Physical therapy and speech therapy
- Note: IBM is treated effectively the same, but has much worse outcomes. There is little evidence that these treatments even do anything.
Most common new-onset myopathy in patients over the age of 50
Inclusion body myositis
Most common reason for a misdiagnosis of an inflammatory myopathy
Erroneous pathologic interpretation of the biopsy
A pathology problem!!!
Overlap myositis
- Any inflammatory myopathy that occurs in association with features of another autoimmune connective tissue disease.
- A classic form of OM is antisynthetase syndrome:
- Characterized by muscle weakness, Raynaud syndrome, nonerosive arthritis, interstitial lung disease, and skin changes to the palms (mechanic’s hands).
- Affected patients are positive for antisynthetase antibodies.

Steroid myopathy
Non-inflammatory, corticosteroid-induced muscle wasting
Presents insidiously in proximal muscle groups with lesser effects on distal muscle groups.
Immune-mediated necrotizing myopathy
An inflammatory myopathy affecting the proximal skeletal muscles that is particularly severe and associated with a markedly elevated CK level. Progresses over weeks to months.
Associated with anti-SRP antibodies, which is the first-line diagnostic test. A anti-SRP negeative form may evolve out of some cases of dermatomyositis
Treatment is largely the same as for other inflammatory myopathies, but outcomes are worse.
-
Stroke69
-
Back to Basics2
-
Essential Tremor13
-
Huntington's Disease19
-
Encephalitis in a Healthy Individual18
-
Parkinson's Disease27
-
Hereditary Neurodegenerative Ataxias17
-
Tardive Dyskinesia and Related Dyskinesias11
-
Acute Spinal Cord Injury15
-
Epidural/Subdural Hematoma6
-
Delirium6
-
Concussions9
-
Lumbar Puncture4
-
Cerebral Cortex I and Vascular Territories49
-
Stroke and Intracerebral Hemorrhage46
-
Seizure and Epilepsy118
-
Subarachnoid Hemorrhage16
-
Stroke in a Young Patient12
-
Peripheral Neuropathy46
-
Syncope and Loss of Consciousness of Unknown Etiology13
-
Psychogenic Nonepileptic Spells7
-
Multiple Sclerosis and Other Myelopathies45
-
Headache55
-
Neuro Exam and Basic Neuro Tips13
-
Approach to Ataxia and Gait Disorders9
-
Alzheimer's Dementia22
-
Lewy Body Dementia18
-
Subacute Combined Degeneration of the Spinal Cord14
-
Optic Neuritis22
-
Acute Disseminated Encephalomyelitis13
-
Meningitis28
-
Botulism19
-
HIV-associated Neurologic Dysfunction/Dementia11
-
Creutzfeld-Jakob Disease18
-
Neurosyphilis24
-
Toxoplasmosis12
-
Sleep Disorders22
-
Pupillary Responses22
-
Pseudotumor cerebri14
-
Diplopia and Oculomotor Palsies8
-
Zoster13
-
Myasthenia20
-
Vertigo12
-
Chronic inflammatory demyelinating polyneuropathy7
-
Guillain-Barre Syndrome17
-
Uncovered High-Yield Topics39
-
Neuro Oncology33
-
Myositides25
-
Amyotrophic Lateral Sclerosis13
-
Anterior Horn Cell Diseases15
-
Febrile Seizure12
-
Muscular dystrophies8
-
Tics and Tourette Syndrome19
-
Benign Rolandic Epilepsy7
-
Lissencephaly13
-
Autism Spectrum Disorder9
-
Cerebellopontine Angle Mass15
-
Wilson's disease4
-
Last Week Prep39
-
Ned Divine Review23
