Classic presentation of tabes dorsalis
- Lancinating pain
- Sensory ataxia
- Hyporeflexia
- Impotence and/or bowel and bladder dysfunction
Rapid plasma reagin
Quite sensitive for primary and secondary syphilis, but NOT for neurosyphilis
Negative RPR does NOT exclude neurosyphilis
Unfortunately, it also frequently has a false-positive result
Venereal diseases tests vs treponemal tests for neurosyphilis
VDRL and RPR are both less sensitive for neurosyphilis than primary or secondary syphilis
However, treponemal tests are both sensitive and specific for all forms of syphilis, including neurosyphilis. If a treponemal test is negative, syphilis has been effectively ruled out.
Typical CSF findings of neurosyphilis
- Elevated CSF protein (up to 200 mg/dL)
- Lymphocytic pleocytosis less than 400/μL
- CSF VDRL positivity most of the time
- Elevated CSF IgG synthesis
If RPR and VDRL are negative but neurosyphilis is still clinically suspected. . .
. . . serum Treponema pallidum-specific antibodies should be performed (aka treponemal tests)
These include:
FTA-ABS, TPHA, MHA-TP
Why don’t we do treponemal tests all the time for syphilis?
They are much more expensive
PCR for syphilis
Unfortunately, this test sucks
Useless. If RPR/VDRL fail, you should just go to treponemal tests instead.
Serologic tests for syphilis cannot distinguish between. . .
. . . syphilis, pinta, and yaws
Pinta and yaws are nonveneral treponemal endemic diseases
Pain in neurosyphilis vs viral sensory ataxia-cranial neuropathy syndromes
In viral etiologies (HIV, Hep B, Hep C), pain is burning
In syphilis, pain is lancinating (stabbing)
Argyll Robertson pupils
Small pupils that constrict when focusing, but fail to constrict when exposed to a bright light. Often bilaterally miotic and irregular at baseline.
In other words, they are reactive to accomodation, but not to light
Classically caused by neurosyphilis. Can also rarely occur in MS, Wernicke’s encephalopathy, diabetes mellitus, Lyme, sarcoid.
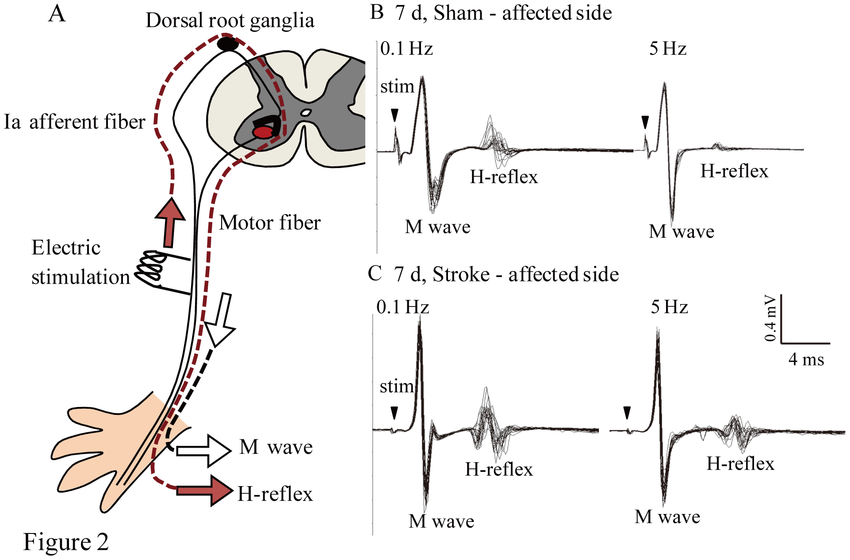
H reflex
Electrical equivalent to a monosynaptic stretch reflex
Reflects pathology along the afferent and efferent fibers and/or the dorsal root ganglion
Primary, secondary, and tertiary syphilis
Primary: Skin or mucocutaneous lesion at the site of infection
Secondary: Disseminated skin or mucocutaneous lesions reflecting syphilitic bacteremia
Tertiary: Neurosyphilis or Tree bark aorta. May occur years later.
Classic exam findings of neurosyphilis
- Argyll Robertson pupils
- Hyporeflexia
- Symptoms localizing to the dorsal column
- Often some cranial nerve abnormalities
Features of syphilitic meningitis
- ~1-2 years following initial infection
- Cranial mononeuropathies
- Hydrocephalus
- Focal hemispheric signs
Syphilitic cerebrovascular-meningovascular disease
- 5-7 years after infection
- Ischemia, particularly in MCA
- Meningeal irritation
- Can present w/ stroke in evolution
Tabes dorsalis typically occurs ___ following initial infection with syphilis
Tabes dorsalis typically occurs >10 years following initial infection with syphilis
Gummatous neurosyphilis
- Form of neurosyphilis that may occur much earlier following syphilis infection
- Effectively a gumma that is compressing the brain – as such it occurs as part of secondary syphilis
- Presents like any brain tumor
Considerations in the ddx for tabes dorsalis
- Subacute combined degeneration due to B12 deficiency
- Multiple sclerosis
- Lyme disease
__ on EMG is often lost in neurosyphilis
H reflex on EMG is often lost in neurosyphilis
Due to damage of the DRG
On EMG testing, __ are selectively affected in neurosyphilis. __ strongly suggests against a diagnosis of neurosyphilis.
On EMG testing, sensory neurons are selectively affected in neurosyphilis. Motor neuron abnormalities strongly suggest against a diagnosis of neurosyphilis.
Treatment of neurosyphilis
- Standard therapies
- High-dose IV aqueous penicillin G for 10-14 days
- If penicillin allergic, doxycycline for 28 days AND ceftriaxone for 14 days should be administered together
- If pregnant AND penicillin allergic, desensitize to penicillin, then treat with penicillin
- If symptoms persist, retreat
- CSF studies should be re-examined after completion of therapy and demonstrate a drop in WBC count, protein, and IgG synthesis
Neurosyphilis in patients with HIV
Neurosyphilis may present much more rapidly in patients with coinfection of syphilis and HIV
As such, take into account risk factors for HIV when considering your DDx. Also, if a patient has clear onset of neurosyphilis with an accelerated timecourse, you should test for HIV.
Patients with neurologic symptoms and a history of syphilis should be assumed. . .
. . . to have neurosyphilis until proven otherwise
Syphilitic aseptic meingitis
Occurs as a chronic infection
Onset 1-2 years after primary infection
May involve headaches, cognitive changes, and cranial nerve abnormalities
-
Stroke69
-
Back to Basics2
-
Essential Tremor13
-
Huntington's Disease19
-
Encephalitis in a Healthy Individual18
-
Parkinson's Disease27
-
Hereditary Neurodegenerative Ataxias17
-
Tardive Dyskinesia and Related Dyskinesias11
-
Acute Spinal Cord Injury15
-
Epidural/Subdural Hematoma6
-
Delirium6
-
Concussions9
-
Lumbar Puncture4
-
Cerebral Cortex I and Vascular Territories49
-
Stroke and Intracerebral Hemorrhage46
-
Seizure and Epilepsy118
-
Subarachnoid Hemorrhage16
-
Stroke in a Young Patient12
-
Peripheral Neuropathy46
-
Syncope and Loss of Consciousness of Unknown Etiology13
-
Psychogenic Nonepileptic Spells7
-
Multiple Sclerosis and Other Myelopathies45
-
Headache55
-
Neuro Exam and Basic Neuro Tips13
-
Approach to Ataxia and Gait Disorders9
-
Alzheimer's Dementia22
-
Lewy Body Dementia18
-
Subacute Combined Degeneration of the Spinal Cord14
-
Optic Neuritis22
-
Acute Disseminated Encephalomyelitis13
-
Meningitis28
-
Botulism19
-
HIV-associated Neurologic Dysfunction/Dementia11
-
Creutzfeld-Jakob Disease18
-
Neurosyphilis24
-
Toxoplasmosis12
-
Sleep Disorders22
-
Pupillary Responses22
-
Pseudotumor cerebri14
-
Diplopia and Oculomotor Palsies8
-
Zoster13
-
Myasthenia20
-
Vertigo12
-
Chronic inflammatory demyelinating polyneuropathy7
-
Guillain-Barre Syndrome17
-
Uncovered High-Yield Topics39
-
Neuro Oncology33
-
Myositides25
-
Amyotrophic Lateral Sclerosis13
-
Anterior Horn Cell Diseases15
-
Febrile Seizure12
-
Muscular dystrophies8
-
Tics and Tourette Syndrome19
-
Benign Rolandic Epilepsy7
-
Lissencephaly13
-
Autism Spectrum Disorder9
-
Cerebellopontine Angle Mass15
-
Wilson's disease4
-
Last Week Prep39
-
Ned Divine Review23
